






Henry Yoder had 10–12 cows out of the tank every single day. Same barns, same crew, same seven‑day treatments on repeat. Then he stopped reaching for the tubes first.

When Henry Yoder looked at his treatment logs for More‑To‑Do Farms’ 1,100 Holsteins in Wisconsin, he didn’t see a mastitis “program.” He saw the same cows cycling through seven‑day antibiotic treatments, over and over, with 10–12 cows out of the tank every single day. That’s a lot of milk in the hospital pen instead of on the milk check.
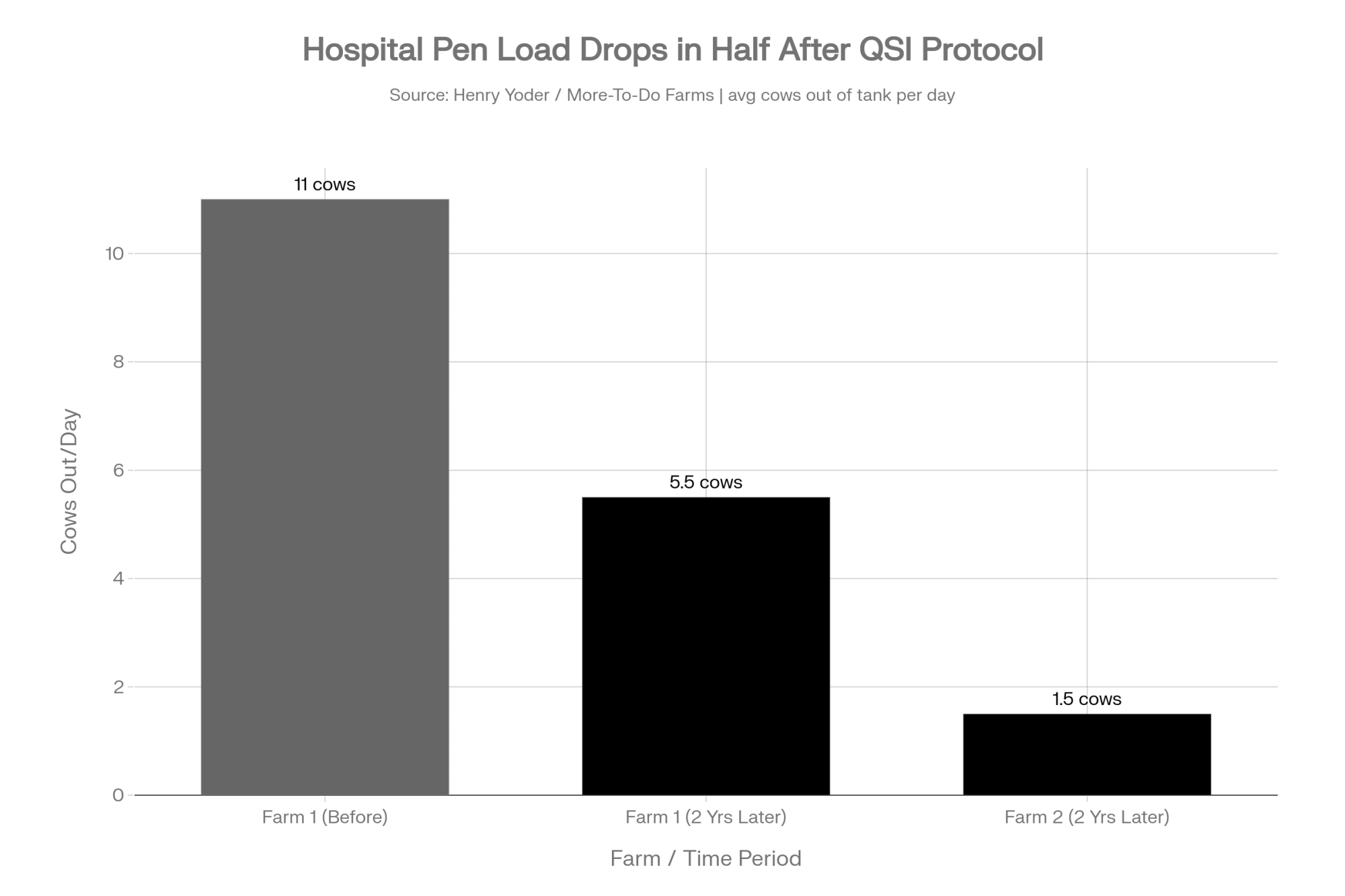
Two years later, Henry’s numbers look very different. Mastitis treatments are down 50–75%, hospital cows dropped to 5–6 a day, treatment duration shrank from seven days to two or three, and one barn has held bulk tank SCC under 100,000 for two straight months — on sawdust, not sand.
This isn’t a story about a magic new tube. It’s about changing what you aim at: biofilm‑protected udder infections that antibiotics alone were never designed to solve, and a different way to think about mastitis economics when replacement heifers are sitting around $3,000 a head.
What Changed on Henry’s Farm — And Why It Matters
Henry manages two Holstein dairies under the More‑To‑Do Farms umbrella in Wisconsin — about 1,150 milking and dry cows across two milking sites, plus roughly 650 head of heifers raised by a custom grower. The business was founded by Doug Knoepke in 1978 and has grown into a seven‑site operation united by a simple mission: “Passionate with Integrity and Ingenuity, for Our People, Our Cows, and Our Land.”
On paper, Henry’s herd looked solid. Cows were monitored with smaXtec boluses, which flag health problems via changes in internal temperature and rumination, roughly 24 hours before your milkers would spot them. His crew was steady. Stalls were clean. Milk was headed to Grassland for butter starting January 15, so every pound counted.
But the mastitis log told a different story. Cows were getting seven‑day courses of Spectrum SLC, clearing up, then flaring again a month later with the same quarter hot and the same cow back in red bands. Across the two dairies, they still averaged 10–12 cows out of the tank every day.
“We are not here to milk a cow for three years. We want long‑term cows that are going to be here for 10 years.” — Henry Yoder.
So Henry did something uncomfortable: he changed the order of operations. Instead of reaching for antibiotics first, he put AHV’s quorum sensing inhibition (QSI) boluses in front of the drug cabinet and let smaXtec call the shots on which cows to touch.
What’s Really Driving These Chronic Mastitis Cases?
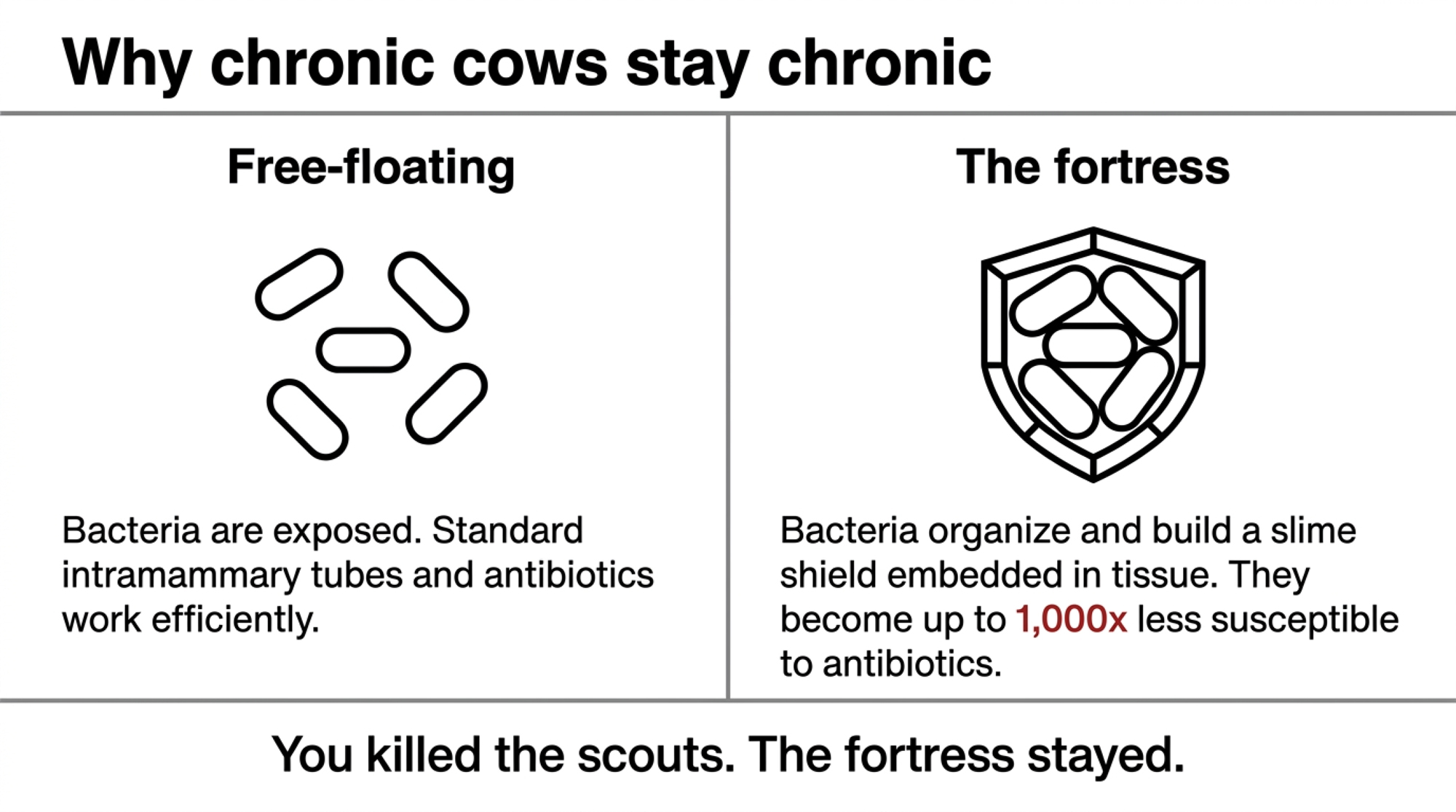
You already know the basics. When bacteria first hit an udder, they’re floating free — planktonic — and that’s where your intramammary tubes do their best work.
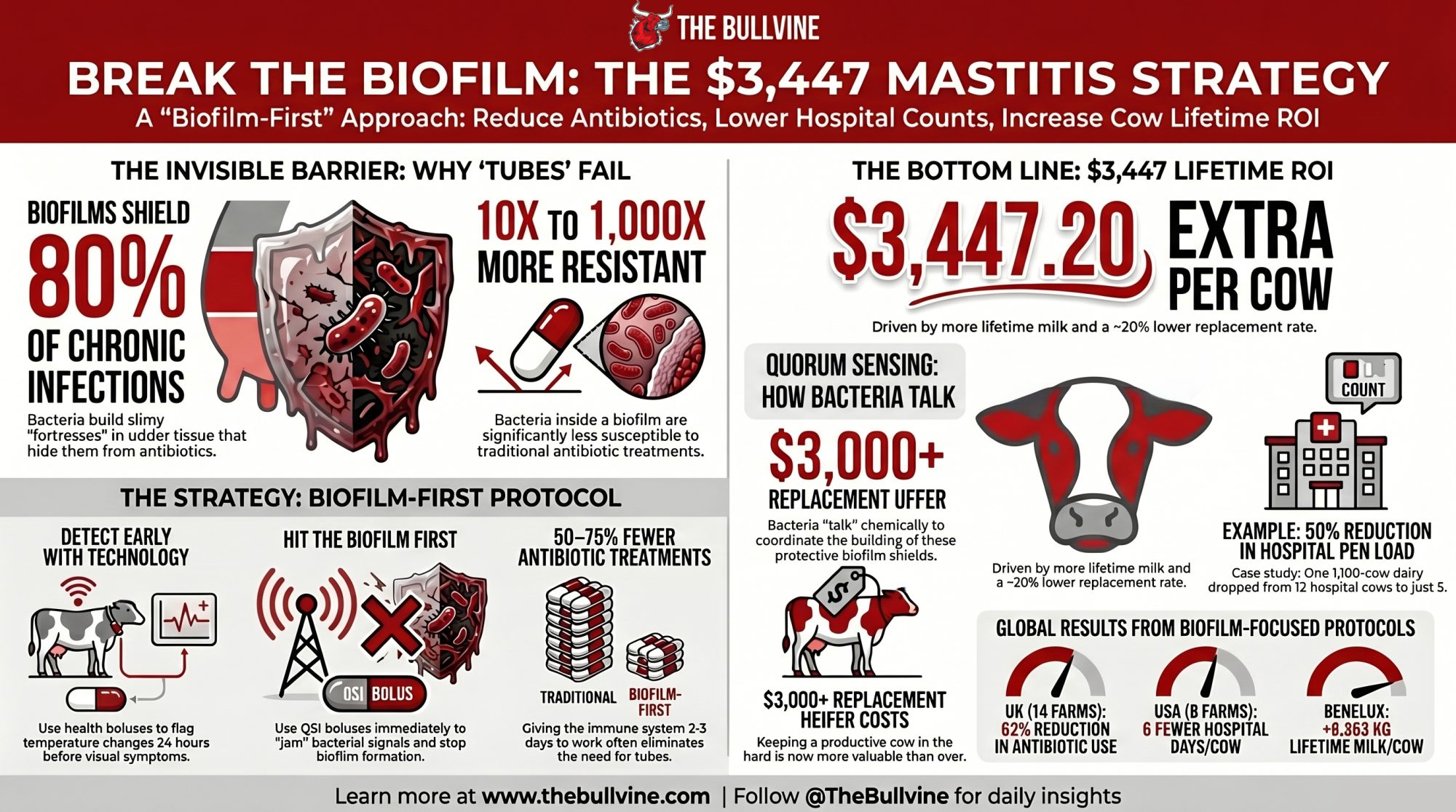
Trouble starts when those bacteria get organized. Through quorum sensing, they “talk” to each other chemically. When enough of them are present, they build a biofilm: a slimy, protective fortress embedded in udder tissue that shields them from immune cells and antibiotics.
Here’s the ugly part:
- Bacteria inside a biofilm can be 10–1,000 times less susceptible to antibiotics than the same strain floating free.
- Biofilms are involved in roughly 80% of chronic and recurrent infections in people and animals.
So when you treat that high‑SCC cow and she looks good for a month, then blows up again after calving or a pen move, it’s not always “treatment failure.” Often, it’s biofilm success. You killed the scouts. The fortress stayed.
Henry saw it in his own barn: “If you use a certain drug for years and years and years, they’ve got to build some resistance to it. … With Spectrum, all of a sudden you’re treating her three times in a lactation.” With the AHV protocol, he says, “there are very few cows that we treat with Spectrum twice in their lactation.”
That’s the pattern this QSI approach is trying to break.
How Does Quorum Sensing Inhibition Fit In?
AHV’s whole play is built around quorum‑sensing inhibition — essentially jamming the communication channelsbacteria use to organize and form biofilms.
Instead of trying to force more antibiotics through the fortress, AHV’s boluses use plant‑derived compounds to disrupt bacterial signaling. Knock out communication, and bacteria can’t coordinate biofilm formation or switch on their virulence genes. They stay exposed, and the cow’s immune system has a fair shot again.
Dr. Gertjan Streefland, AHV’s founder and chief science officer, puts it in barn‑language:
“If you have a group of nasty people, you blindfold them and make them deaf. They cannot communicate anymore. So you’re immediately harmless.”
External RTI lab work backs up the lab‑side claims: AHV’s patented compounds inhibit biofilm formation in field bacteria from both gram‑positive and gram‑negative species, with no resistance development detected in their tests. Because you’re not killing bacteria directly — you’re disabling their communication — there’s less selective pressure for resistance.
That’s the science layer. The question is whether it actually moves the needle in real barns like yours.
What Did Henry Actually Change Day‑to‑Day?
Henry didn’t throw out antibiotics. He just stopped letting them be the first move every time a cow blipped.
Here’s his current play on mastitis‑type alerts:
- Step 1: Let the tech holler first. smaXtec flags a health problem — usually a temperature or rumination change — often a full day before anyone in the parlor would have noticed.
- Step 2: Hit biofilms first. The flagged cow gets an AHV Quick bolus right away, followed by Aspi. That’s the first line of defense now, not the last.
- Step 3: Wait 2–3 days. They give the cow’s immune system time to work with the bolus. If she clears, they never open the antibiotic drawer. If she doesn’t, then they treat — but it’s the exception, not the rule.
“Before, they were treating these cows for seven days,” Henry says. “All of a sudden, they were treating these cows for two to three days, and then back in the tank. Then we put the protocol in that they’re going to wait two to three days after the pill before we start treating. After that, all of a sudden, we hardly had any treated cows.”
He still leans on the broader udder‑health protocol — Quick, Extra, Aspi, and Booster — around high‑risk windows like dry‑off and the first weeks fresh. But the everyday story is simple: detect early, hit biofilms first, only reach for tubes if you still need them.
There’s also a human piece. “Nobody likes treating the cow,” Henry says. “Anytime we don’t have to treat a cow and put red bands on it, it is a positive thing.” More‑To‑Do doesn’t run a separate sick‑cow pen, so fewer treated cows also mean fewer chances for withheld milk to sneak into the tank.
| Step | Old Protocol (Antibiotic-First) | New Protocol (Biofilm-First) | Why It Changed |
|---|---|---|---|
| Detection trigger | Milker spots clinical signs in parlor | smaXtec temp/rumination alert ~24 hrs early | Earlier catch = smaller biofilm load |
| First intervention | 7-day Spectrum SLC intramammary course | AHV Quick bolus + Aspi immediately | Target biofilm communication, not just planktonic bacteria |
| Wait window | Treat continuously for 7 days | Wait 2–3 days; let immune system work | Antibiotic decision made after biology has a chance |
| Antibiotic decision | Default YES on day 1 | Only if cow doesn’t turn corner by day 3 | Exceptions, not the rule |
| Avg treatment duration | 7 days | 2–3 days | Fewer withhold days, less labor |
| Retreatment rate | Same cow, same quarter, multiple times/lactation | Rare second treatment per lactation | Biofilm disruption reduces cycling |
| Cows out of tank | 10–12/day | 5–6/day (Farm 1); 1.5/day (Farm 2) | Hospital pen nearly eliminated on Farm 2 |
| Milk dumped risk | High (red bands on multiple cows daily) | Low (red band cows are an exception) | Fewer chances for a missed band to dump a tank |
Micro Barn Math: What Did That Change Put Back in the Tank?
Let’s run Henry’s numbers with today’s price deck so you can map it to your own herd.
USDA’s March 2026 WASDE pegs the 2026 all‑milk price at $19.70/cwt, down about $1.47 from 2025’s revised average of $21.17.
On Henry’s first farm, he went from 10–12 cows out of the tank daily to 5–6 cows. Call it 5.5 cows recovered on an average day.
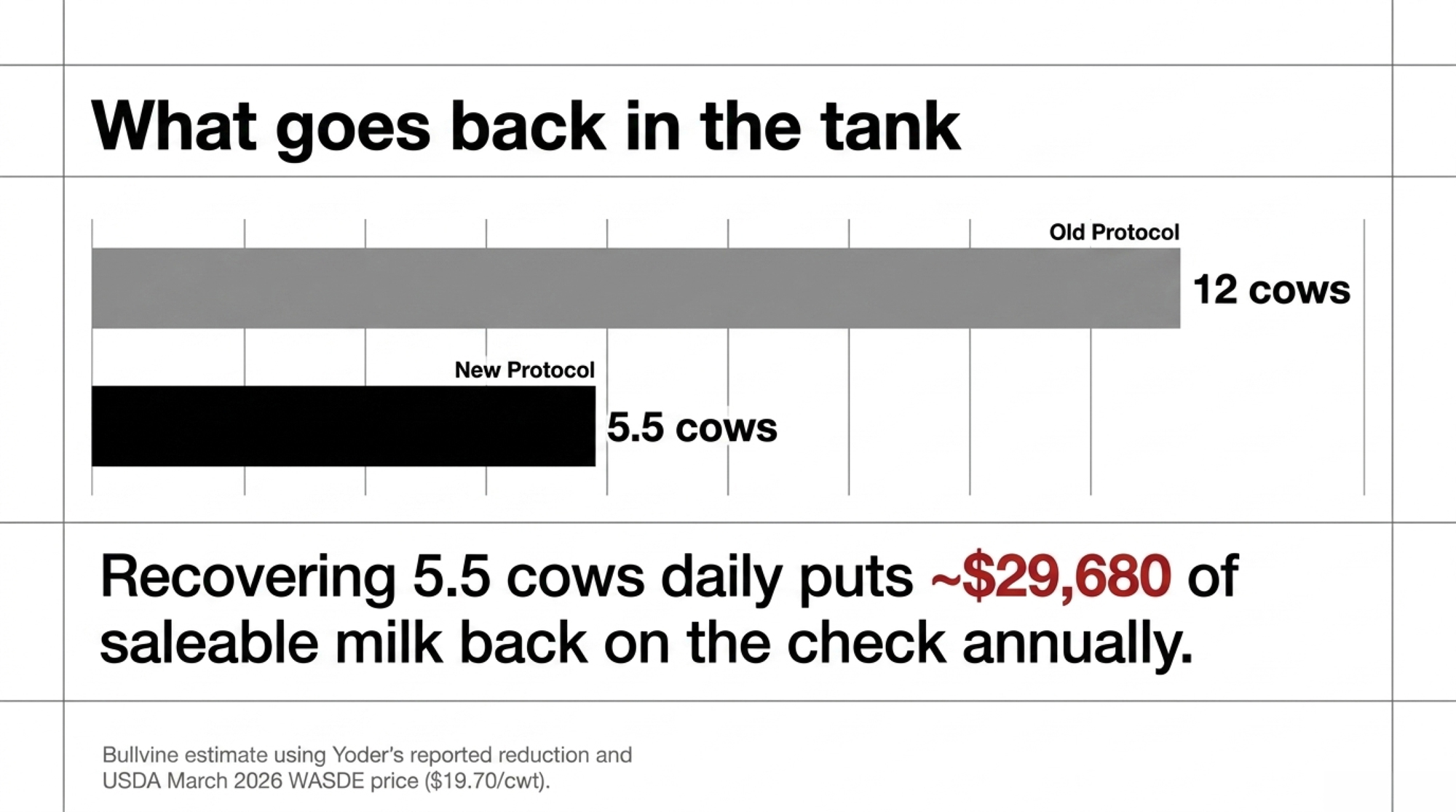
Assume:
- 75 lbs/day per cow.
- At $19.70/cwt, that’s $0.197 per lb.
- Each recovered cow puts 75 × $0.197 ≈ $14.78/day back into saleable milk.
- Over a year: 5.5 cows × $14.78 × 365 ≈ $29,680 of milk that used to live in the hospital pen. (Bullvine estimate using Henry’s reported reduction and USDA March 2026 WASDE price.)
That’s just the recovered milk, not counting fewer tubes, less labor catching treated cows, or the risk of dumping a whole tank if someone misses a leg band.
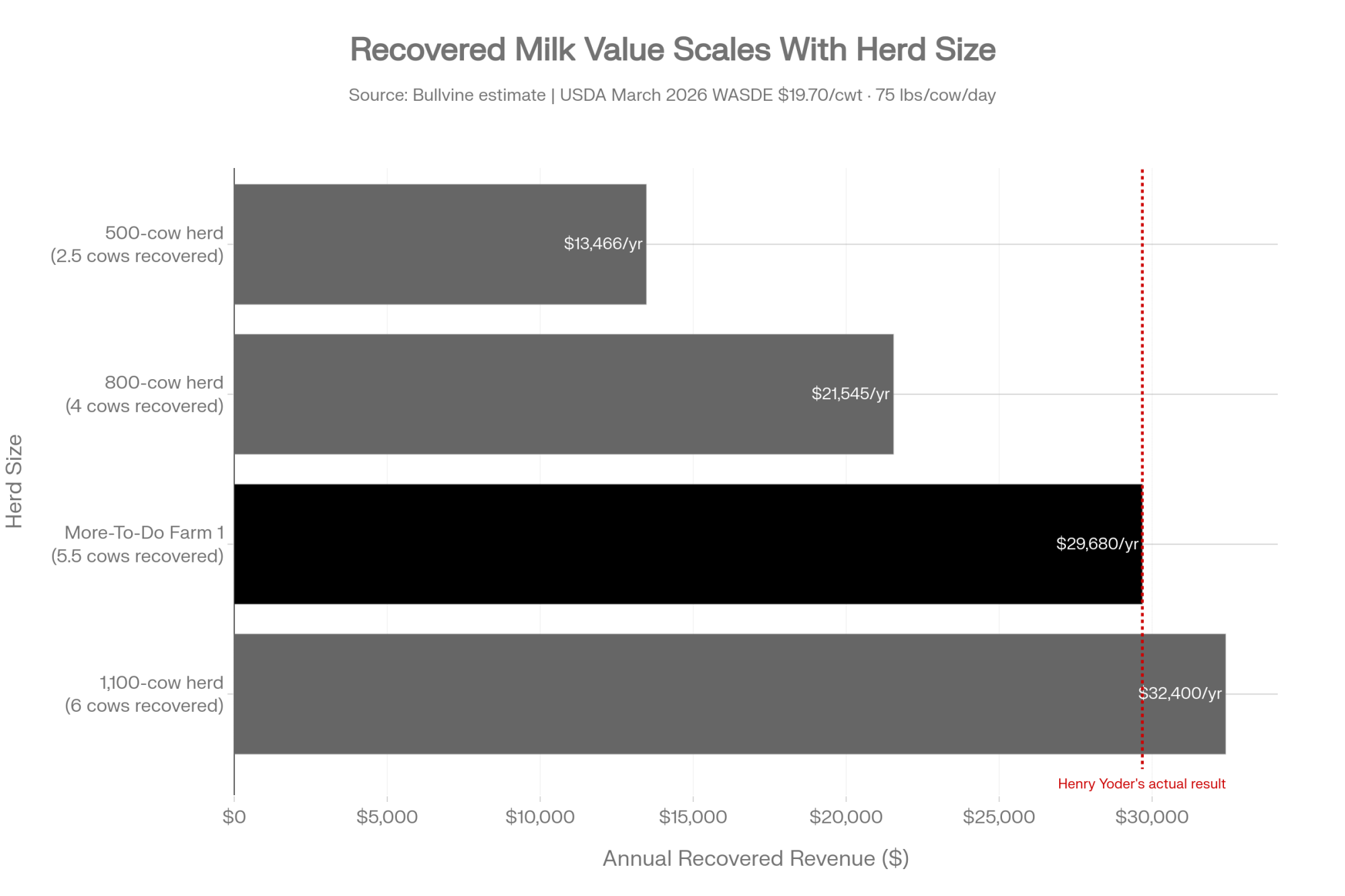
On Henry’s second site — 570 cows — he’s averaging just 1.5 cows out of the tank on a given day. That’s less than 0.3% of the herd. He actually has to pull some high‑SCC cows from the tank to have enough whole milk to feed calves — a problem you don’t hear often.
Now scale that down. If you’re a 500‑cow herd with, say, 5 cows out of the tank most days, and you cut that in half, you’re recovering roughly:
- 2.5 cows × $14.78/day × 365 ≈ $13,500/year in milk alone.
You can plug in your own pounds and price, but the shape of the math won’t change much.
How Big Is the Mastitis Hole in Your Own Budget?
You already know mastitis isn’t cheap. But putting some numbers around it helps you decide whether a protocol shift is worth the fight.
A few benchmarks:
- Bovine mastitis is estimated to cost the global dairy sector up to $35 billion a year.
- Dr. Pam Ruegg’s work on 37 Wisconsin dairies (averaging ~1,300 cows) found per‑case clinical mastitis treatment costs ranging from $120 to $330 for essentially the same disease, depending on how the farm managed days treated and drug choices.
- In that same dataset, 83% of farms treated clinical mastitis longer than the label allows — meaning a big chunk of cost was self‑inflicted.
Now overlay today’s replacement math.
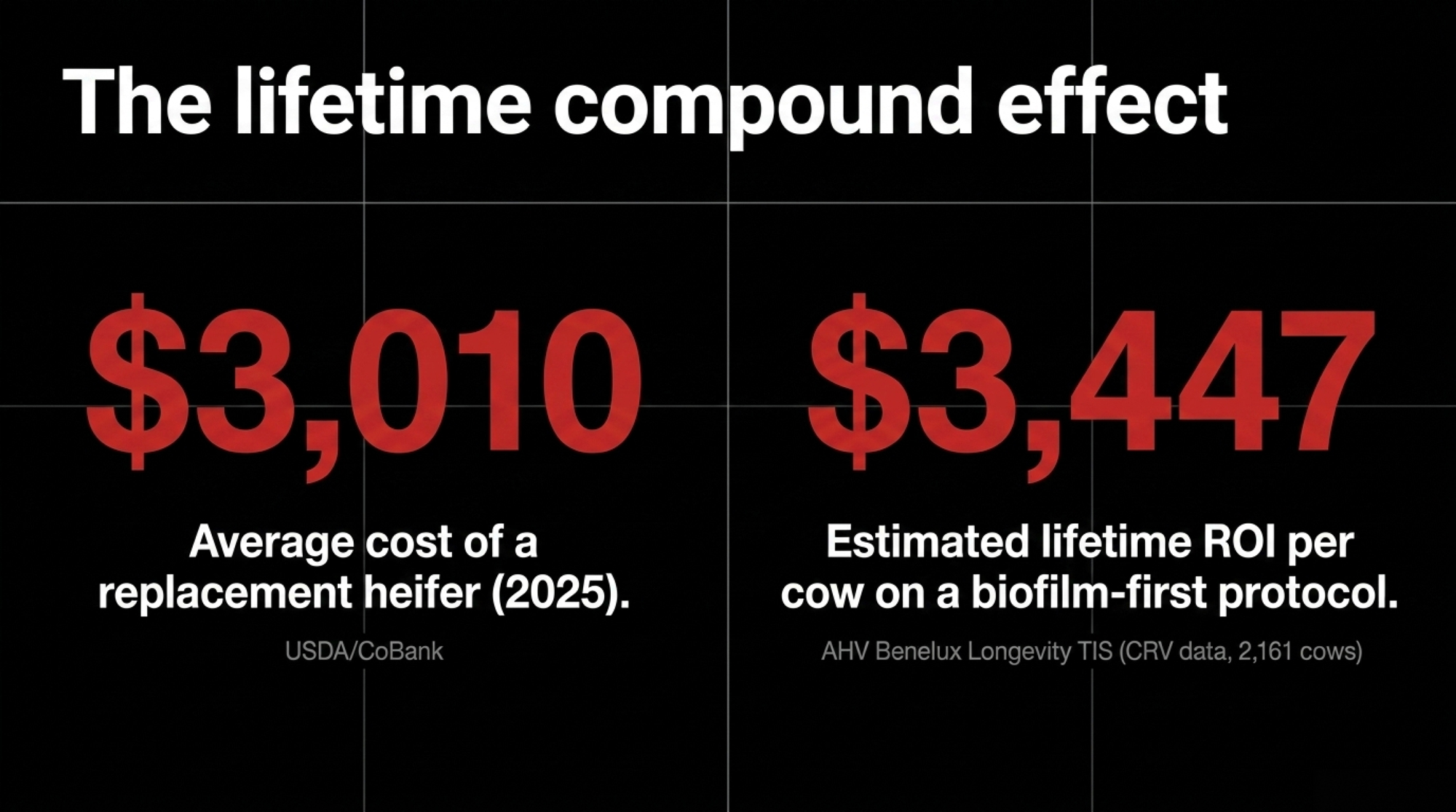
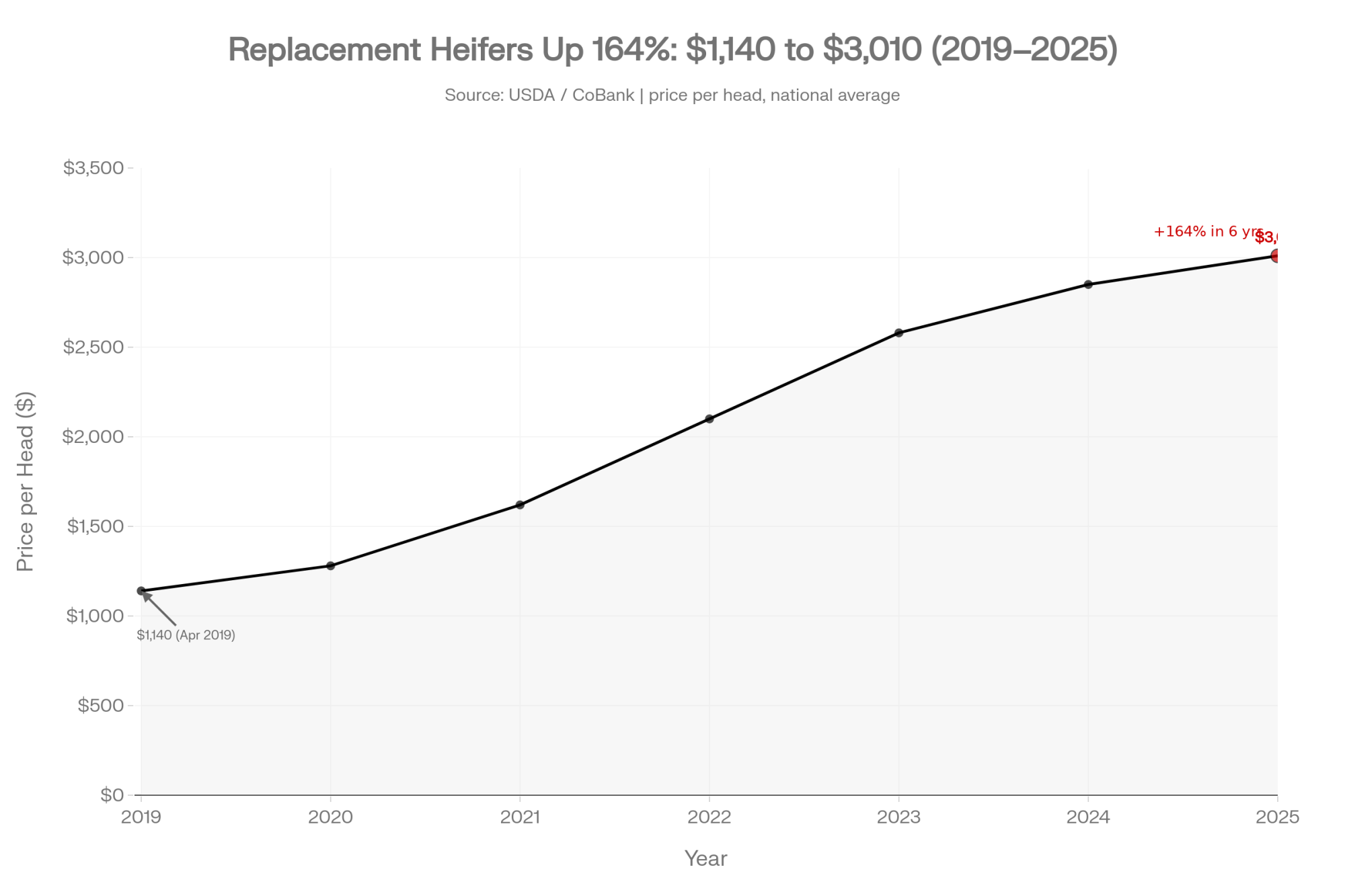
USDA and CoBank data show replacement heifers hitting about $3,010 per head in July 2025 — up roughly 164%from around $1,140 in April 2019. Later USDA estimates pushed that as high as $3,110 in late 2025 before backing off slightly, but top heifers in some regions still clear well above that.
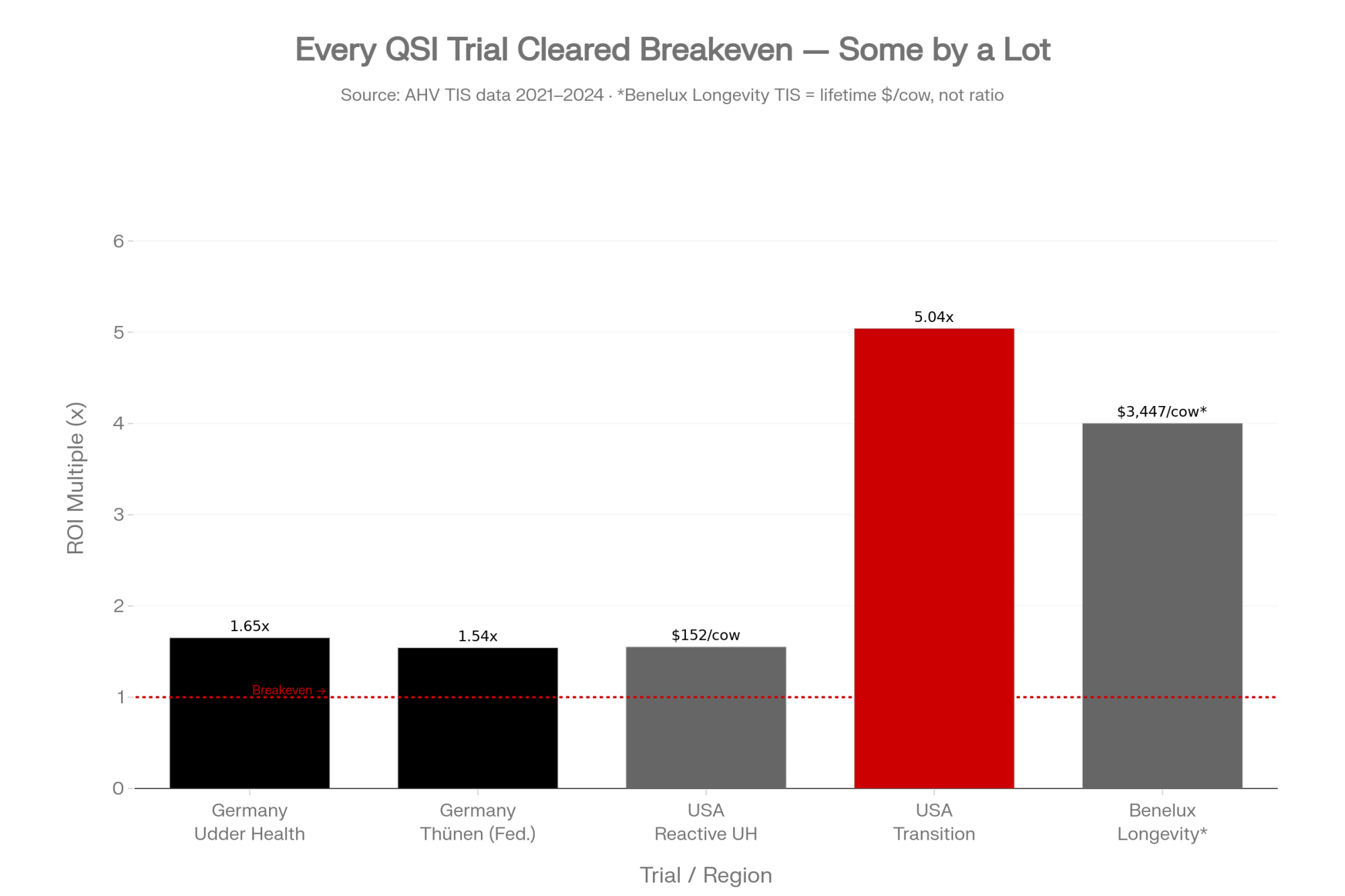
According to AHV’s Benelux Longevity TIS, a multi‑farm dataset of 2,161 cows built on CRV records, the protocol works out to a lifetime ROI of $3,447.20 per cow, tied to:
- 8,653 kg more lifetime milk per cow.
- About €0.44 more revenue per day of life.
- A 19.8% lower replacement rate compared to Dutch CRV averages.
That’s not Henry’s own ROI sheet; it’s a multi‑farm European dataset. But it tells you this much: if you can safely keep cows productive longer and keep them out of the hospital pen, the compound economics are very real.
Can Other Farms Really Reproduce What Henry Is Seeing?
No two herds are the same. But Henry isn’t the only one seeing this kind of shift. AHV’s trial and field data, plus farm stories from different regions, point in the same general direction: less antibiotic use, fewer repeats, and more years on good cows.
Here’s what’s been measured so far:
| Region | Farms / Cows | Key Results | Source & Timing |
| UK | 14 farms, 2,774 cows | 62% less antibiotic use for mastitis, 42% fewer clinical cases, +29.3% 1st‑service conception | AHV HHP Progress, 2023–2024 |
| Germany | 6 farms, 325 cows | 75.7% drop in SCC (P<0.05), ROI 1.65, ≈€140 per cow | AHV Udder Health TIS, 2021–2022 |
| Germany (Thünen Institute) | 1 farm, 11 cows (pilot) | €1.54 return per €1 invested, ~260.6 kg less waste milk per cow | Federal research institute, 2024 |
| USA (Reactive udder health) | 8 farms, 3,316 cows | 6 fewer hospital days per cow; $151.53 lower cost/cow from less waste milk and labor | AHV TIS, 2022–2023 |
| Benelux (Longevity) | 2,161 cows | +8,653 kg lifetime milk, €0.44 more per day, 19.8% lower replacement, $3,447.20 ROI/cow | AHV Benelux Longevity TIS, based on CRV data |
| USA (Transition & Fertility) | 8 farms, 4,495 cows | +3.2 kg/day milk first 100 DIM, −34% metritis, ROI 5.04 (~$160.76 per cow) | AHV Transition/Fertility TIS, 2024 |
There’s also an independent trial you’ll want to watch: Texas A&M’s SARE project OS24‑178, “Evaluating a Non‑antibiotic Treatment of Mastitis in Organic Dairy Cows.” The project calls for about 120 lactating Holsteins in a Texas organic herd, randomized to AHV vs. organic standard care, with bacteriology, PCR, and SCC performed at TAMU.
That’s the kind of third‑party data vets like Ruegg have been asking for. Results are still pending. Until they land, you’re looking at:
- Company‑associated multi‑farm field data.
- A small but credible federal pilot (11 cows at Thünen).
- Real‑world stories like Henry’s and Karl Gabrielse at Quonset Farms, where fresh cow problems dropped from 20% to 2% and conception rates climbed 6 points after implementing AHV protocols.
It’s not a slam‑dunk RCT portfolio yet. But it’s enough signal that serious producers are at least testing QSI, not just dismissing it outright.
Is the $3,447 ROI Number Something You Can Bank On?
You shouldn’t bank on anyone’s ROI number — ours, AHV’s, or your neighbor’s — without running your own. But you can use it as a reference point.
The $3,447.20 per cow comes from AHV’s Benelux Longevity TIS, built on CRV data across 2,161 cows. It represents extra lifetime milk, fewer replacements, and more revenue per day of life. It’s an average across many herds in a European system, not a guaranteed outcome for your barn in Wisconsin, Ontario, or New York.
Treat it like a sire proof:
- Directionally useful.
- Needs to be filtered through your milk price, your cull rate, and your vet’s comfort level.
If you want the deep dive on how longevity, replacement cost, and cull‑rate math actually stack up, that’s a follow‑up article on its own.
What Does This Look Like Operationally in Your Barn?
Switching any protocol — AHV or otherwise — creates friction. You’re asking people to change how they’ve done things for years.
Based on Henry’s experience and the trial data, you can expect a few things if you go down this road:
- Less time in the hospital pen. AHV’s US reactive udder‑health TIS showed 6 fewer hospital days per cow, and Henry’s own numbers match that direction.
- Shorter treatment windows. Seven‑day courses turned into two‑to‑three‑day interventions, often without tubes at all.
- Fewer withhold headaches. Fewer drugged cows mean fewer chances for a red‑band miss to turn into a dumped tank.
- Higher bar for milker prep. Henry is blunt: “It’s everything hand in hand. It’s on the milkers too — they have to do a good job of prepping. Clean stalls, everything plays hand in hand.”
If your stalls are sloppy and your prep is inconsistent, no bolus in the world is going to bail you out. Quorum sensing inhibition is a layer, not a shortcut past basic udder hygiene.
How Bad Is Your Udder Problem Really, and Is It Worth Changing Protocols?
First move is boring and free, but it’s the one most farms skip: audit your own records.
In the next 30 days, sit down with your DHIA reports and cull log and do three things:
- Calculate udder‑related culls for the past 12 months.
- What percentage of involuntary culls are tagged to mastitis, high SCC, or udder health?
- If you’re north of 20%, you’ve probably got a structural udder‑health issue, not just bad luck.
- Count your average hospital‑pen load.
- On a typical day, how many cows are out of the tank?
- If more than 1–1.5% of your herd lives there, you’re leaving more on the table than you think.
- Pick three “problem cows” and follow the money.
- How many times have you treated each this lactation?
- How many days was each cow out of the tank per treatment?
- Are they still in the string or on a truck?
Once you see those numbers on paper, you’ll know if a biofilm‑first approach is worth trialing — or if you’re mostly dealing with basics you can tighten up without changing products.
| Metric | Green Zone | Yellow Zone | Red Zone — Act Now | Henry’s Farm 1 Start |
|---|---|---|---|---|
| Udder-related culls (% of involuntary culls) | < 10% | 10–20% | > 20% | Not disclosed |
| Hospital pen load (% of herd on any day) | < 0.5% | 0.5–1.5% | > 1.5% | ~1.0% (10–12 of 1,100) |
| Avg treatment duration per clinical case | ≤ 3 days | 4–6 days | 7+ days | 7 days |
| Cow retreatment rate (same quarter, same lactation) | Rare (<1/cow/yr) | Occasional | Cycling repeaters on your list | Same cows monthly |
| Bulk tank SCC (cells/mL) | < 100,000 | 100,000–200,000 | > 200,000 | Not disclosed (Farm 2 now < 100k) |
| Replacement heifer cost (current regional price) | < $2,000 | $2,000–$2,500 | > $2,500 | ~$3,010 (national avg, July 2025) |
If You Try a Biofilm‑First Protocol, Where Do You Start So It Doesn’t Blow Up in Your Face?
If your audit says, “Yeah, we’ve got an udder problem,” the next question is where to start without turning the barn upside down.
Best candidates for a trial:
- Chronic repeaters you’re already thinking about culling.
- High‑SCC cows caught early by monitoring systems (SCR, smaXtec, activity collars) before a quarter blows up.
- Herds where stalls and prep are decent, but the same cows keep showing up on the treatment list.
Henry’s path looked like this:
- Add smaXtec (or use what you already have) for early alerts.
- When an alert hits, reach for Quick + Aspi first, not tubes.
- Give it 2–3 days and let the cow’s immune system work with the bolus.
- Only bring in antibiotics if she doesn’t turn the corner.
The big operational risk is confusion. Your team has to know:
- Which cows are “AHV only.”
- Which cows are on antibiotics.
- Exactly when each cow is safe to go back in the tank.
The win is when “red‑band” cows become the exception — not a daily pattern your milkers are numb to.

Sponsored Post
Options and Trade‑Offs for Farmers
Path 1: 30‑Day Paper Audit (No Products, Just Records)
When it makes sense: If you don’t actually know your udder‑related cull rate or your average hospital‑pen load, this is your starting line.
What it requires:
- One afternoon with your DHIA reports, cull records, and a notepad.
- Maybe your lender, vet, or nutritionist on the phone for a second set of eyes.
What you get:
- A clean “here’s where we stand” view on udder‑related culls, hospital‑pen load, and retreatment patterns.
- The ability to plug your numbers into any ROI discussion — whether it’s AHV, a different product, or just tightening milking routines.
If your numbers are already good — low udder culls, low hospital counts, stable SCC — you may decide you’re doing enough. If they’re rough, at least you know you’re not imagining it.
Path 2: 90‑Day Pilot on Your Worst Group
When it makes sense: If your audit shows a clear udder problem and you’ve got a handful of chronic cows chewing up labor and drug spend, but you’re not ready for a whole‑herd flip.
What it requires:
- Agreement with your herd vet on which cows qualify and how you’ll track them.
- A written protocol — for example, “AHV Quick + Aspi on first alert, wait 2–3 days, then decide on antibiotics.”
- Clean notes on SCC, hospital days, and total treatments over those 90 days.
What it costs:
We do know from German and US TIS data that:
- In Germany, AHV’s udder‑health protocol showed an ROI of 1.65 and about €140 per cow benefit, driven by lower SCC and less waste milk (AHV Udder Health TIS, 2021–2022).
- In US reactive udder‑health trials, farms saw 6 fewer hospital days per cow and about $151.53 per cow in reduced costs between waste milk and labor (AHV TIS, 2022–2023).
Risks and limits:
- If your basics are weak, you might not see much improvement.
- If your team isn’t on board, partial compliance will muddy the waters and make the trial look “inconclusive.”
At the end of 90 days, you should know if your chronic problem cows are still chronic — or if you’ve actually broken the cycle.
Path 3: 12‑Month Whole‑Herd Strategy Shift
When it makes sense: If you’ve nailed the basics, your hospital pen is still busier than you like, and you’re serious about pushing cows to fifth lactation and beyond — the way Henry is aiming for 20% of his herd there.
What it requires:
- Full buy‑in from your vet, herd manager, and parlor crew.
- A clear written protocol around dry‑off, fresh cows, and “alert” cows.
- The patience to let biology catch up to your ideas — you’re changing the baseline, not flipping a switch.
Upside:
- Higher probability of hitting the kinds of numbers seen in the AHV Benelux Longevity TIS — more older cows, lower replacement pressure, more milk per day of life.
- A different relationship with antibiotics, which matters as regulations and consumer expectations tighten around antimicrobial use.
Risks and limits:
- You’re betting on company‑associated data plus one small independent pilot and an in‑progress Texas A&M trial. The science of biofilms is solid, but product‑specific proof is still developing.
- If milk prices or replacement markets swing again, the economics of longevity can shift too.
This is not a “set it and forget it” option. It’s a management philosophy change.
Key Takeaways
- If more than ~20% of your culls are udder‑related or more than 1–1.5% of your herd lives in the hospital pen, you’ve got a structural udder‑health problem. Start with the 30‑day record audit before you try to buy your way out of it.
- If the same cows keep cycling through mastitis treatments, there’s a good chance biofilms are part of your problem. That’s when it makes sense to at least pilot a biofilm‑first protocol with your vet, whether it’s AHV or another approach.
- If replacement heifers are running in the $3,000 ballpark in your region, every cow you keep productive for one more lactation is worth a second look. Longevity‑driven ROI like the $3,447/cow figure (AHV Benelux Longevity TIS) comes from compounding effects — more older cows, fewer replacements, more milk per day of life — not just drug savings.
- If your stalls are dirty, your prep is inconsistent, or your milking system is out of tune, fix those first. No QSI bolus, no matter how clever, will outrun bad basics. Even Henry is clear: the science helps, but it rides on cow comfort and routine.
You don’t have to be sold on AHV for this article to matter. You have to answer some uncomfortable questions about how many cows you’re really losing to udder health and how much milk is living in your hospital pen instead of on your milk check.
Henry didn’t change because of a white paper. He changed because his own numbers wouldn’t shut up.
In the meantime, pull your records, count your hospital cows, and ask yourself a simple question:
What would your barn feel like if half the red‑band cows disappeared from the string next month — for the right reasons?
Complete references and supporting documentation are available upon request by contacting the editorial team at editor@thebullvine.com.
Learn More
- Robotic Milking & Mastitis: The Hidden Profit Killer in Your Barn — Overcome the unique udder health obstacles of automated systems with five targeted management strategies. This implementation guide exposes why subclinical mastitis drains $662 per cow annually and outlines the exact protocols to salvage leaking margins.
- The $3,000 Heifer Hangover: How Beef‑on‑Dairy Emptied Your Pipeline and Left the U.S. 800,000 Head Short— Position your business for the next three years by dissecting the historic replacement heifer shortage squeezing the industry. This analysis breaks down the national inventory collapse and arms you with critical regional data to reshape your culling strategy.
- The $1700 Longevity Paradox: How One 1700-Cow Dairy Cut Udder Culls in Half — Disrupt conventional culling habits with an inspection of multi-farm, peer-reviewed data tracking biofilm intervention. This case study details how a massive 23% reduction in culling probability can add $1,700 in lifetime profit per cow.
 The Sunday Read Dairy Professionals Don’t Skip.
The Sunday Read Dairy Professionals Don’t Skip.
 The Sunday Read Dairy Professionals Don’t Skip.
The Sunday Read Dairy Professionals Don’t Skip.Every week, thousands of producers, breeders, and industry insiders open Bullvine Weekly for genetics insights, market shifts, and profit strategies they won’t find anywhere else. One email. Five minutes. Smarter decisions all week.
