Seven of Cornell’s 24 SDCT herds bailed on the program once their fresh‑cow mastitis numbers hit the fan. Before you join them, you’d better know which group you’re in.
Executive Summary: Herds trying selective dry cow therapy at 240,000 SCC can easily turn “antibiotic savings” into a $6,920 loss on 300 cows once extra mastitis, culls, and lost milk are in the math. Cornell’s 24‑herd SDCT project cut dry‑cow antibiotic use 53% on average, but 7 herds still abandoned SDCT when fresh‑cow mastitis and milk quality slipped. Dutch data shows dairy can cut antimicrobial use roughly 47% without wrecking udder health, but only after years of tightening SCC, housing, and protocols. This piece lays out three realistic paths for higher‑SCC herds under processor pressure: fix infections first, pilot SDCT on the safest slice only, or use that SDCT letter as leverage for a 12–18‑month runway. You’ll see the exact SCC thresholds, AABP readiness criteria, and barn‑math assumptions so you can plug in your own DHIA and cull numbers. If your bulk tank’s been north of 200,000 and your mastitis records are patchy, you’ll likely walk away treating SDCT as a future goal, not a box to tick this dry‑off season.

When The Bullvine first profiled Mystic Valley Dairy’s move to selective dry cow therapy, one detail jumped off the page: a bulk tank somatic cell count around 78,000 cells/mL and a decision to start skipping dry‑cow tubes on some cows anyway.
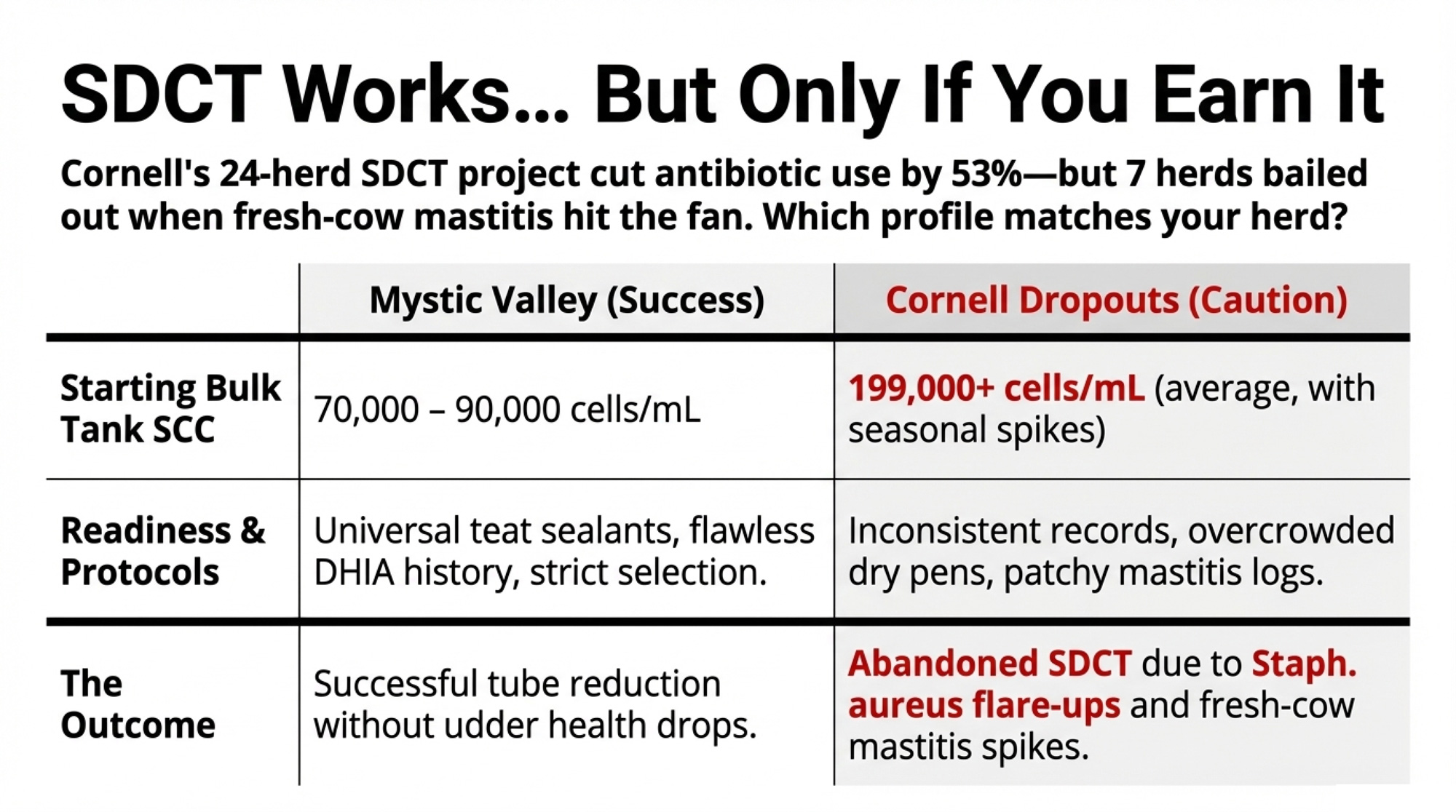
Around the same time, Cornell’s Quality Milk Production Services team was quietly tracking 24 New York herdsthrough their own SDCT transition. Those farms averaged 199,000 cells/mL SCC going in and still managed to cut dry‑cow antibiotic use by 53% on average (range: 32–78%) without wrecking udder health. Put those two stories beside a 240,000‑SCC herd with a processor letter on the kitchen table, and the contrast gets real fast.
Mystic Valley’s SDCT Story: Low SCC, High Scrutiny
Mystic Valley Dairy, Sauk City, Wisconsin, milks about 450 registered Holsteins, with a bulk tank SCC typically ranging from 70,000 to 90,000 cells/mL. In The Bullvine’s earlier coverage, owner Mitch Breunig laid out why a herd with that kind of SCC profile would even consider cutting dry‑cow tubes.
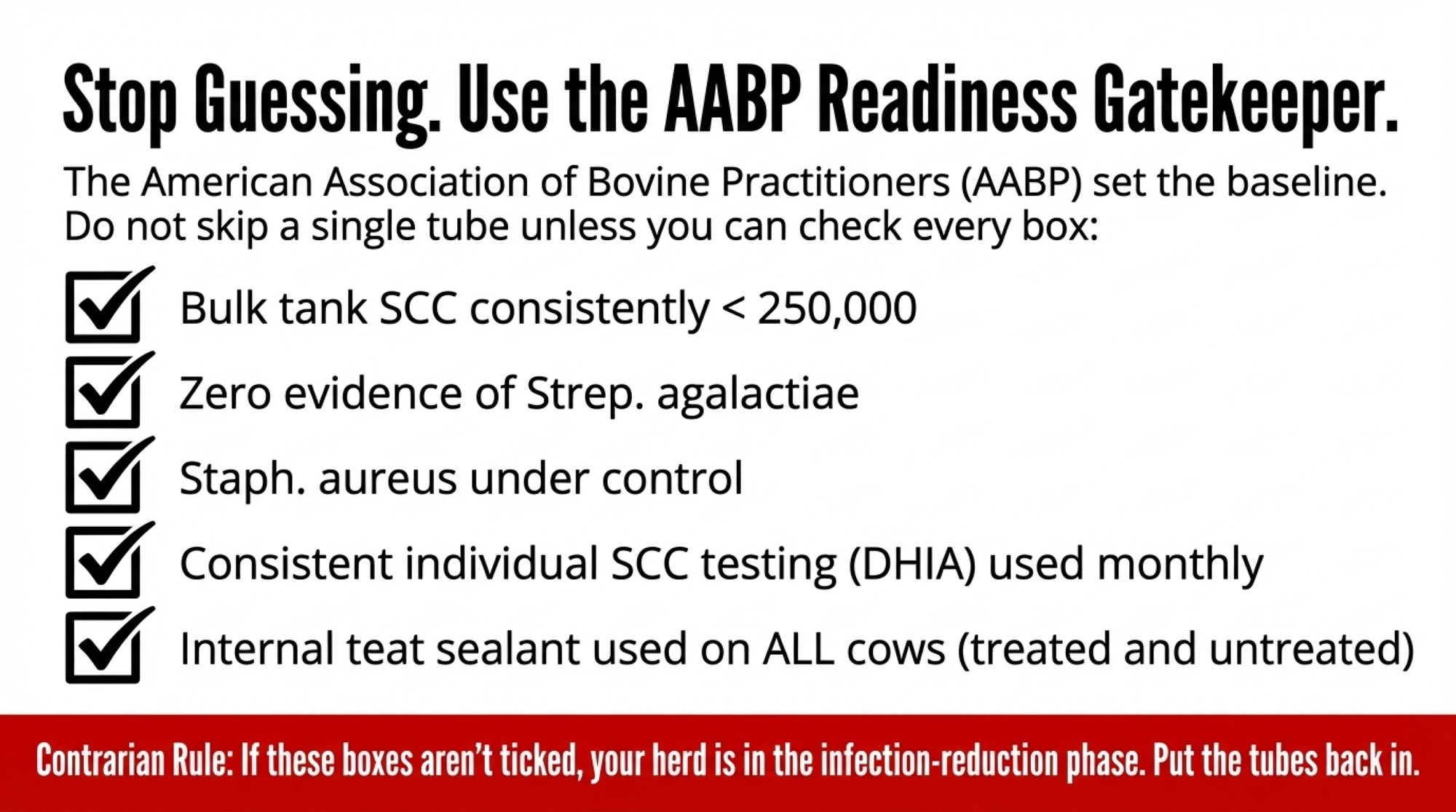
Mystic Valley already ticked every box in the 2024 AABP SDCT readiness guidelines and then some: bulk tank SCC regularly less than 250,000; no evidence of Streptococcus agalactiae; Staphylococcus aureus under control; consistent individual SCC testing; written milking and dry‑off SOPs; and internal teat sealant at dry‑off for all cows. On paper, they looked a lot like the 12 Flemish herds in Lipkens, Piepers, and De Vliegher’s 2023 trial, which had a geometric mean bulk tank SCC of 145,000 cells/mL at enrollment (range: 84,000–195,000; median 157,000) and used teat sealants on every dry cow.
Mystic Valley’s criteria were conservative from the start: cows needed three straight SCC tests under 200,000, no clinical mastitis during the lactation, no flagged problem quarters, and a good‑eyes‑on udder check at dry‑off before they were considered for sealant‑only treatment. Everyone else stayed on full dry‑cow therapy plus sealant.
Even in that low‑SCC, well‑run context, Mystic Valley still saw some early‑lactation cows whose performance raised eyebrows. Those early outcomes led the farm and its vet to tighten criteria further and pay closer attention to which cows truly belonged in the sealant‑only column.
The point isn’t that SDCT was easy for them. It’s that they were operating from a starting point — and with protocols — most 240,000‑SCC herds don’t have yet.
Cornell’s 24 SDCT Herds: 53% Fewer Tubes, Not for Everyone
If Mystic Valley shows what SDCT looks like on a very low‑SCC herd, Cornell’s New York project shows what happens when you put it into a broader mix of operations.
| Readiness factor | Mystic Valley Dairy | 240,000‑SCC herd under pressure |
|---|---|---|
| Bulk tank SCC (cells/mL) | 70,000–90,000; long‑term <150,000 | 240,000+; bounces 230,000–280,000 |
| Individual SCC data | 3 consecutive tests <200,000 required for SDCT cows | Patchy DHIA; high‑SCC cows not consistently flagged |
| Contagious pathogens | No Strep. ag; Staph. aureus under control | Staph. aureus “suspected” or intermittently cultured |
| Dry‑off protocol | Written SOP; one named dry‑off lead; sealant for all cows | Shared between milkers; protocol drift between shifts |
| Teat sealant use | 100% of dry cows receive internal teat sealant | Used on “problem cows” only or inconsistently |
| Housing & dry pens | Stocking density and bedding managed; low overcrowding (implied by low SCC) | Overcrowded, wetter pack; limited capital for upgrades |
| AABP 2024 SDCT checklist | Ticks every box and more | Fails multiple criteria; SDCT pushed by processor, not data |
Potter, Forrestal, Capel, and Nydam’s 2022 AABP paper followed 24 commercial dairy farms across New York State. Herd sizes ranged from 65 to 3,774 cows, averaging 985 cows, with a starting bulk tank SCC of 199,000 cells/mL. Farms worked with veterinarians to use individual cow SCC and mastitis history to decide who received full dry‑cow therapy plus sealant and who received sealant only, and then monitored bulk tank SCC, fresh‑cow SCC, and clinical mastitis as they transitioned.
Across those 24 herds:
- 53% average reduction in dry‑cow antimicrobial use (individual herds ranged from 32% to 78%).
- No consistent herd‑level spikes in fresh‑cow SCC or mastitis when SDCT was implemented inside the project’s framework.
- 17 of the 24 farms still used SDCT at the end of the study period.
- 7 farms stopped SDCT, citing seasonal milk‑quality challenges, more dry‑period clinical mastitis, or flare‑ups of contagious pathogens such as Staph. aureus.
Cornell didn’t treat SDCT as a universal good or an obvious mistake. They treated it as a tool that fit most of those herds — but not all — even with structured support and monitoring. For a 240,000‑SCC herd being pushed toward SDCT, that nuance matters more than the headline number.
When Selective Dry Cow Therapy (SDCT) Helps — and When It Bites
The published science lines up with what Mystic Valley and Cornell saw.
A 2000–2021 systematic review and meta‑analysis found that selective dry cow therapy can deliver udder‑health outcomes similar to blanket dry cow therapy (BDCT) while reducing antibiotic use — but only in herds with low bulk tank SCC, good mastitis control, and consistent use of internal teat sealants in untreated quarters. Winder et al. (2019, Animal Health Research Reviews) concluded that SDCT increases the risk of intramammary infection at calving compared with BDCT unless internal teat sealants are used; with sealants, IMI risk is similar across strategies.
The Lipkens trial offers a clean real‑world comparison. In those 12 Flemish herds (466 cows; 244 BDCT, 222 SDCT), all cows received an internal teat sealant at dry‑off. Total antimicrobial consumption for udder health between dry‑off and 100 DIM dropped from 1.25 defined course doses (DCD) per cow in the BDCT group to 1.06 DCD per cow in the SDCT group — a 22% reduction — with no significant differences in test‑day SCC, clinical mastitis incidence, milk yield, or culling hazard. Only 33.8% of SDCT‑group cows actually skipped antibiotic tubes at dry‑off, and that share varied widely between herds (6.2–73.9%).
At the national scale, the Dutch experience shows how far antibiotic use can fall when an entire system commits to it. The Netherlands set mandatory reduction targets starting in 2009 and banned preventive antimicrobial use — including blanket dry‑cow treatment — beginning in 2012–2013. Across all Dutch livestock, the result was a 70.8% reduction in kilograms of antimicrobials sold since 2009 (Moura et al., 2022, Frontiers in Veterinary Science). Within the dairy sector specifically, Lam et al. (2020, Pathogens) reported a 47% decline in total antimicrobial usage from 2009 to 2015, after which usage stabilized at around 3 DDDA per cow per year.
Critically, Santman‑Berends et al. (2020, Journal of Dairy Science) monitored approximately 17,000 Dutch dairy herds (about 1.67 million cows) from 2013 through 2017 and found that the ban on blanket dry‑cow therapy drove a 63% drop in dry‑cow antimicrobial usage and a 15% reduction in intramammary treatment overall — with no deterioration in udder health at the herd level. An increase in new high‑SCC cases during the dry period was expected, but as their census data showed, it was not observed.
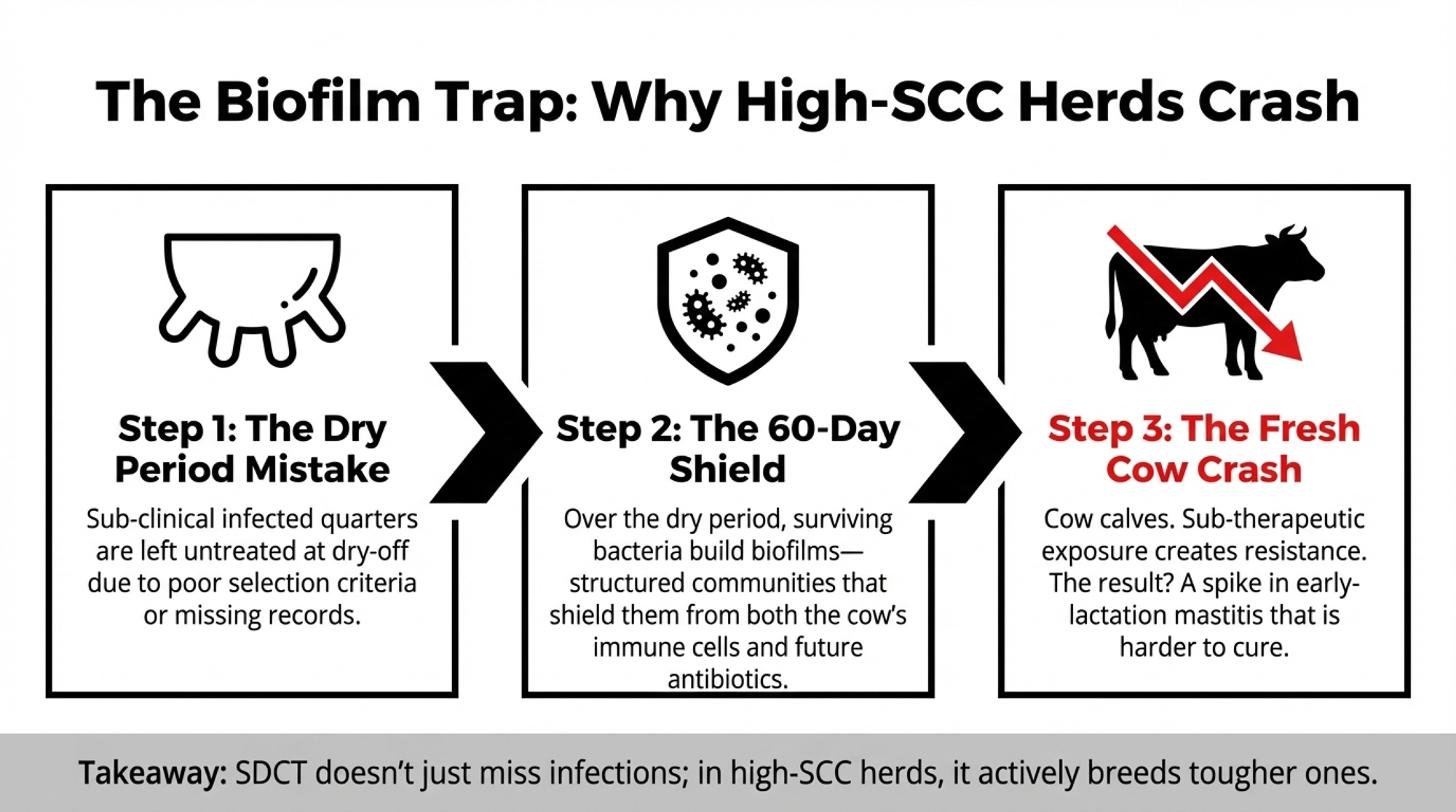
But those same studies underscore a risk that doesn’t appear in tube‑count dashboards: the biofilm and resistance trap. If infected quarters aren’t treated at dry‑off, bacteria have the entire dry period to build biofilms — structured communities that shield them from antibiotics and immune cells. Within those biofilms, resistance genes can move between bacteria more easily via plasmids and mobile DNA elements. When those cows calve and receive intermittent or incomplete lactation treatments, sub‑therapeutic exposure becomes a selection program for resistance.
For low‑SCC herds with solid protocols, that risk is manageable. For a 240,000‑SCC herd with inconsistent records or overcrowded dry pens, it’s a much easier trap to fall into.
Can a 240,000‑SCC Herd Really “Save” on SDCT?
Rollin, Dhuyvetter, and Overton (2015, Preventive Veterinary Medicine) estimated the total cost of a single clinical mastitis case in the first 30 DIM at approximately $444 per case, including lost production, treatment, discarded milk, labour, and culling risk. Other work puts direct costs closer to $120 per case, making a $120–$444 range across studies reasonable.
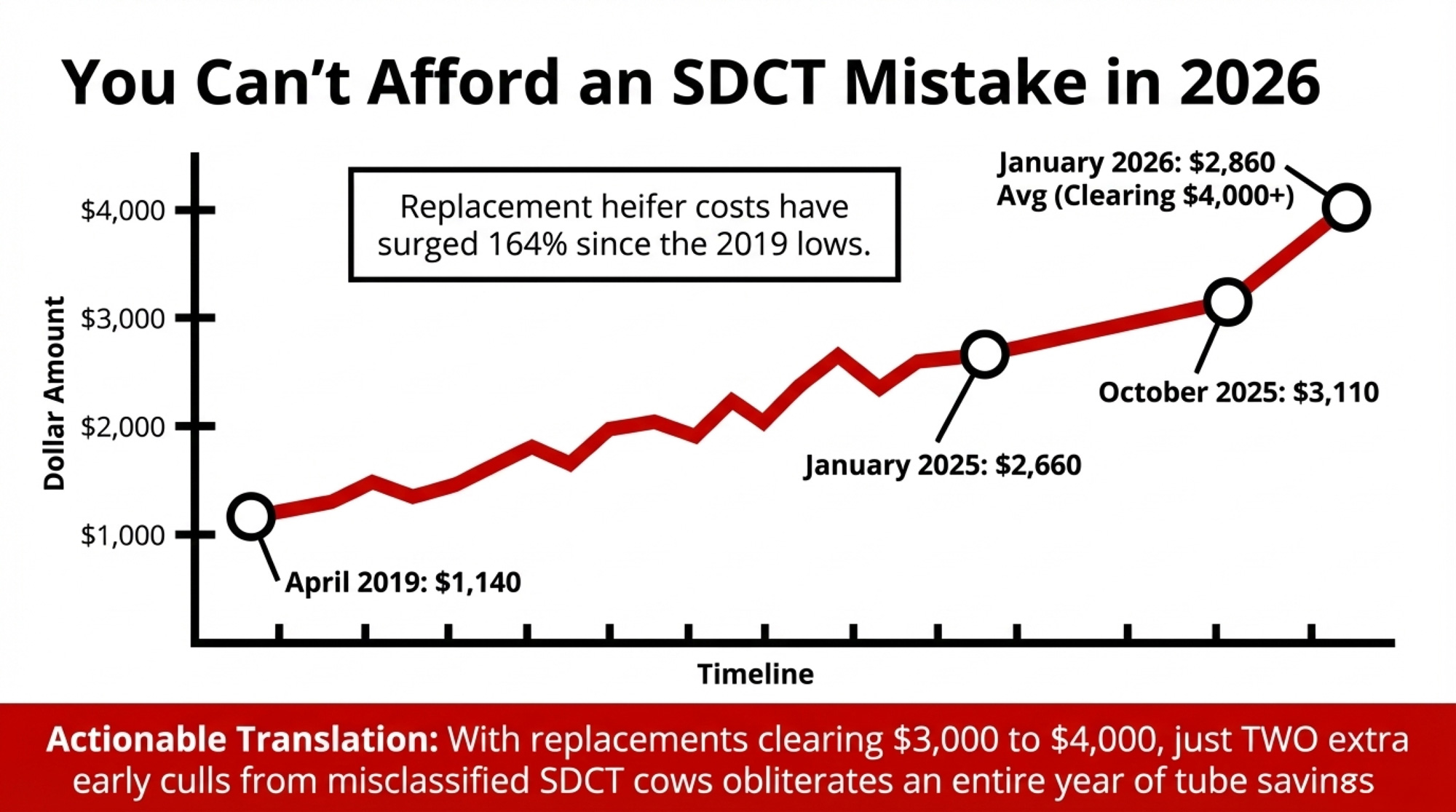
Replacement economics have shifted just as sharply. CoBank and USDA data show:
- October 2014: dairy replacement heifers at $2,120 per head.
- April 2019: down to $1,140.
- January 2025: back up to $2,660.
- July 2025: $3,010.
- October 2025: $3,110 — about a 164% increase from the 2019 low.
- January 2026: USDA average around $2,860, with individual Holstein springers clearing $4,000+ in some California and Midwest auctions.
| Cost item | Conservative value | Cost vs. $1,080 tube “savings” |
|---|---|---|
| Clinical mastitis case (first 30 DIM) | $300 per case (mid‑range of $120–$444)image.jpg | 4 cases = $1,200 (already exceeds tube savings) |
| Sub‑clinical mastitis over lactation | ~$200 lost milk/premiums per cowimage.jpg | 6 cows = $1,200 in hidden loss |
| Net replacement heifer (Jan 2026 avg) | $2,860 − ~$1,400 cull value ≈ $1,500 per headimage.jpg+1 | 1 early cull = 1.4× tube savings; 2 culls = 2.8× |
| High‑end Holstein springer (auction) | $4,000+ per head in some marketsimage.jpg+1 | 1 cull on premium cow = 3.7× tube savings |
| 90 tubes skipped at dry‑off | $12 per tube; total $1,080 “saved”image.jpg | Best‑case upside, before any mastitis or cull penalties |
Now put that together on a 300‑cow herd with a BMSCC around 240,000 that jumps into SDCT before its infection pressure, and records are ready. If your dry‑off person is also your night milker and calf feeder, SDCT will show every crack in that schedule. And if selection criteria or follow‑through miss even a modest number of quiet infections, you can see a bump in early‑lactation mastitis, a couple of cows pushed into earlier culls, and several sub‑clinical cases dragging SCC and milk across the whole lactation.
Here’s what that looks like, using conservative assumptions:
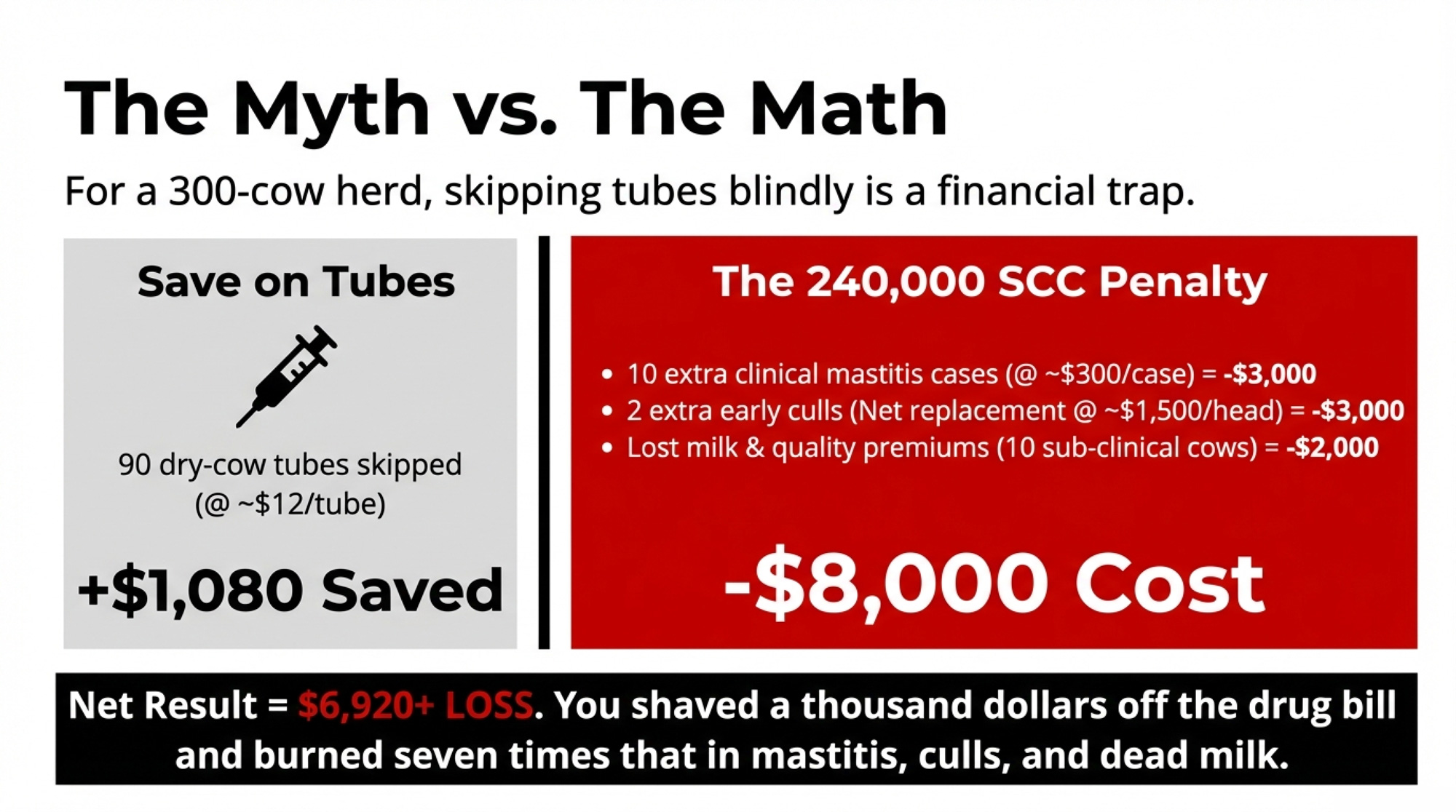
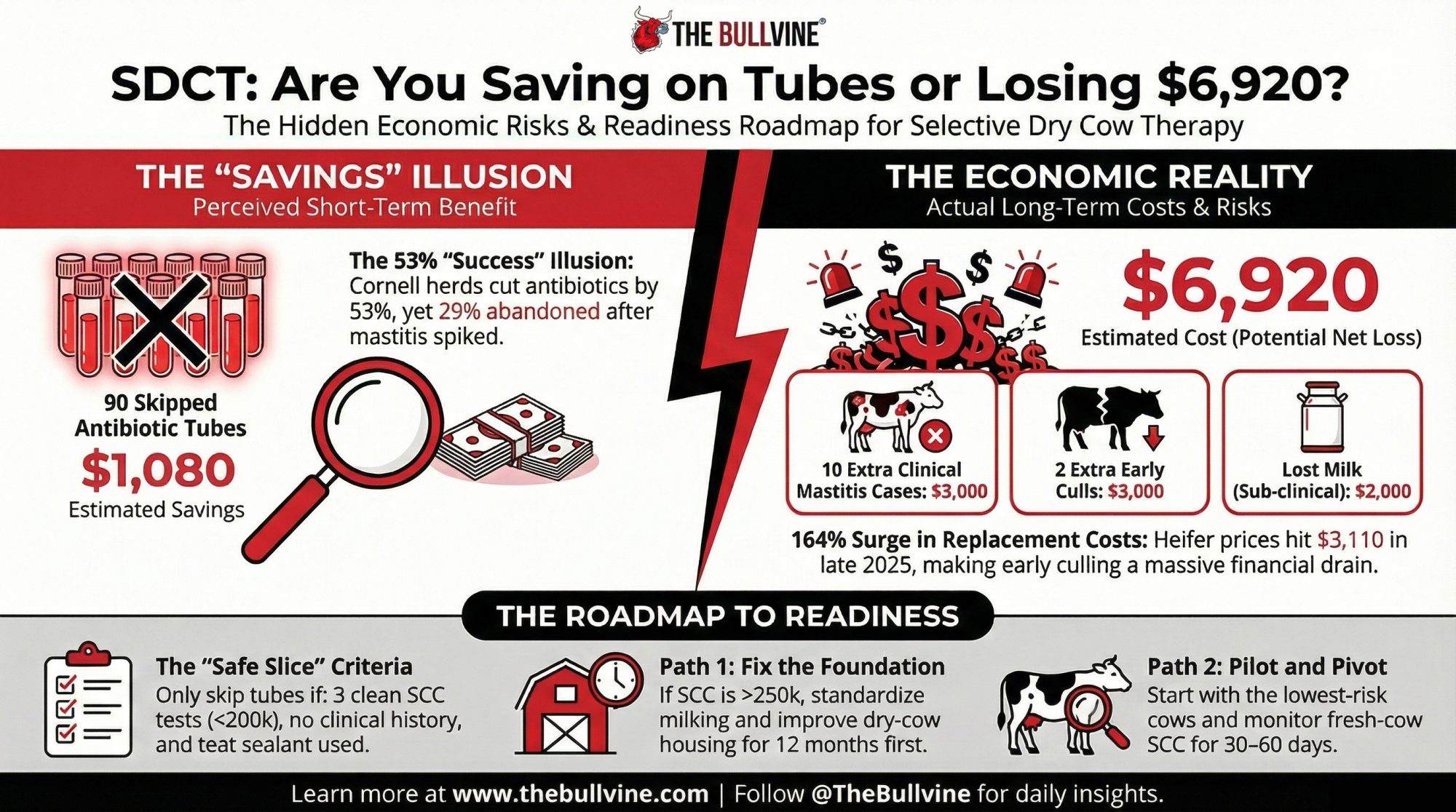
| Item | Savings | Cost |
| 90 dry‑cow tubes skipped (@ ~$12/tube) | $1,080 | — |
| 10 extra clinical mastitis cases (@ ~$300/case) | — | $3,000 |
| 2 extra early culls (net replacement @ ~$1,500/head after cull credit) | — | $3,000 |
| Lost milk from 10 sub‑clinical cows (a few hundred dollars per cow across the lactation) | — | ≈$2,000 |
| Net result | ≈$6,920+ loss |
Assumptions: tubes $8–$15 each (long‑acting dry‑cow products) with $12 used here; mastitis cost $120–$444/case, $300 mid‑range; net replacement cost $2,860 USDA Jan 2026 average minus roughly $1,400 cull cow value ≈ $1,500; sub‑clinical cows losing a few hundred dollars worth of milk and quality premiums per cow across a full lactation.
You’ve shaved about a thousand dollars off your dry‑cow drug bill. You’ve potentially burned seven times that in mastitis, culls, and dead milk.
Mystic Valley’s low SCC, universal sealant use, and disciplined selection meant it could adjust early and keep that risk in check. The Cornell herds that stuck with SDCT had similar structures and data feedback loops. A 240,000‑SCC herd without those pieces is betting $6,920+ a year that its infection status and records are better than they really are.
Three SDCT Paths: Matching the Science to Your Herd
The Mystic Valley and Cornell stories don’t say “don’t do SDCT.” They say “do it on the right herds, with the right prep, and be ready to stop if the data turns.”
For a 240,000‑SCC herd with a processor letter, you’ve got three realistic paths forward.
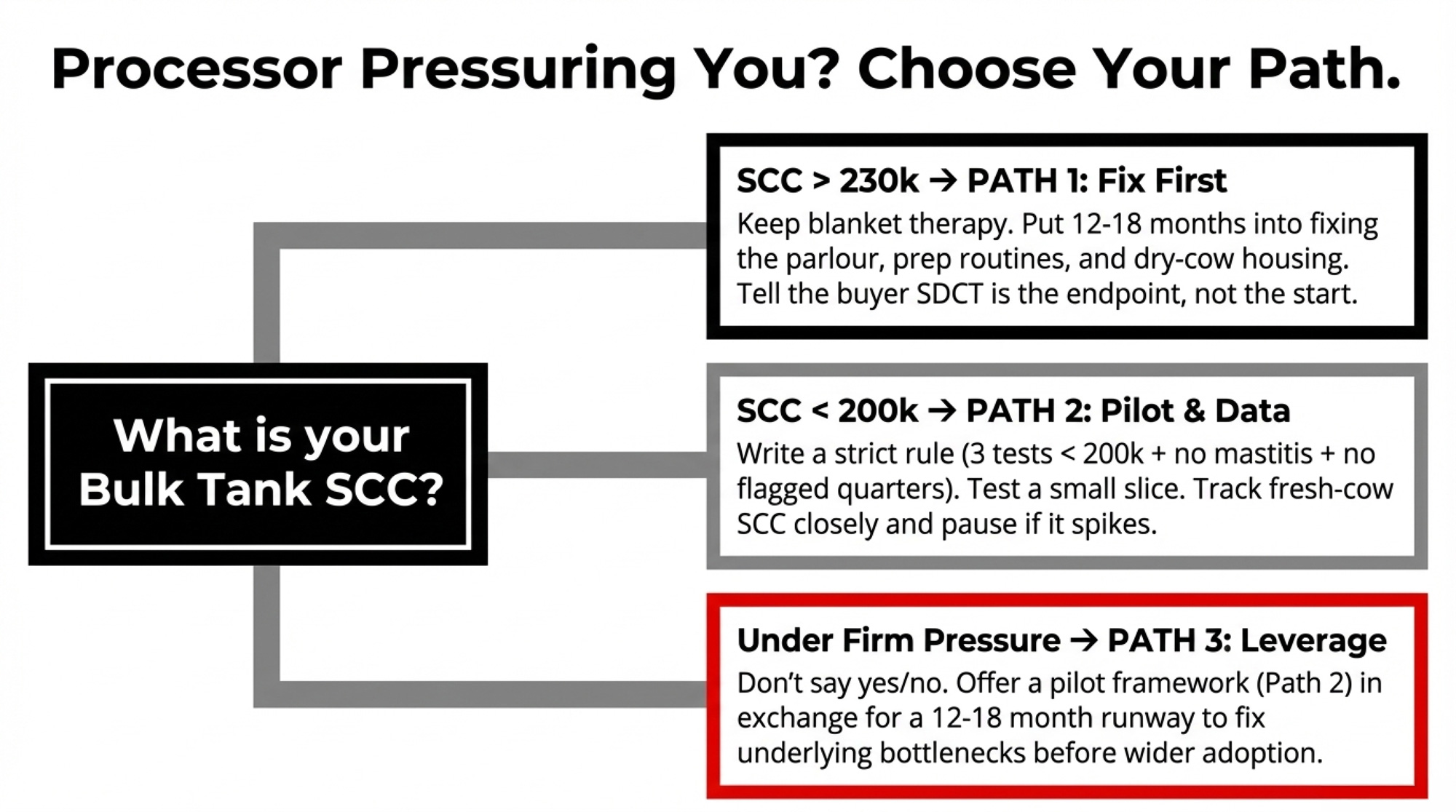
1. Infection‑First: Fix the Foundation Before You Touch Tubes
This fits herds with BMSCC regularly above 230,000–250,000, chronic high‑SCC cows you already know by number, and dry pens that are too full or too wet.
You tell your buyer SDCT is the endpoint, not the starting point. Then you put 12–18 months into:
- Standardizing milking routines: consistent prep, lag time, and post‑dip across every shift; fix drift in technique between employees.
- Tuning the parlour: vacuum levels, pulsation, liners, unit alignment.
- Improving dry‑cow housing: stocking density, bedding, drainage, airflow.
- Culling or segregating chronics instead of carrying them through another lactation.
You stay on blanket dry‑cow therapy plus internal teat sealant for all cows while you do that work. That’s exactly how the AABP 2024 SDCT guidelines recommend sequencing for herds that don’t yet meet readiness criteria. You’re trading short‑term antimicrobial‑use “wins” for long‑term udder‑health and economic stability.
2. Pilot SDCT on the Safest Slice — and Let the Data Decide
This fits herds with BMSCC trending toward 200,000 or below, reasonably clean records, and a willingness to course‑correct.
With your vet, you write a short, strict rule:
- Last three SCC tests all under 200,000.
- No clinical mastitis this lactation.
- No known problem quarters or chronic flags.
Cows that pass become eligible for sealant‑only at dry‑off. Eligibility isn’t a guarantee — if anyone on the crew has doubts about a cow, she stays on full treatment.
Then you monitor:
- Fresh‑cow SCC at first test (5–45 DIM), focusing on the percentage over 200,000.
- Clinical mastitis in the first 60 DIM, clearly tagged by dry‑off treatment group.
The AABP guidelines include specific DairyComp setups to track this. University of Minnesota Extension’s SDCT resources walk through herd‑level readiness and monitoring in plain language. Cornell used similar metrics to sort their 24 herds into “stayed in” and “opted out.”
If your graphs look like the Lipkens and Cornell success herds — stable SCC, no disproportionate mastitis spike among sealant‑only cows — you can cautiously widen eligibility. If they start to look like the seven Cornell herds that stopped, close the gate and go back to Path 1.
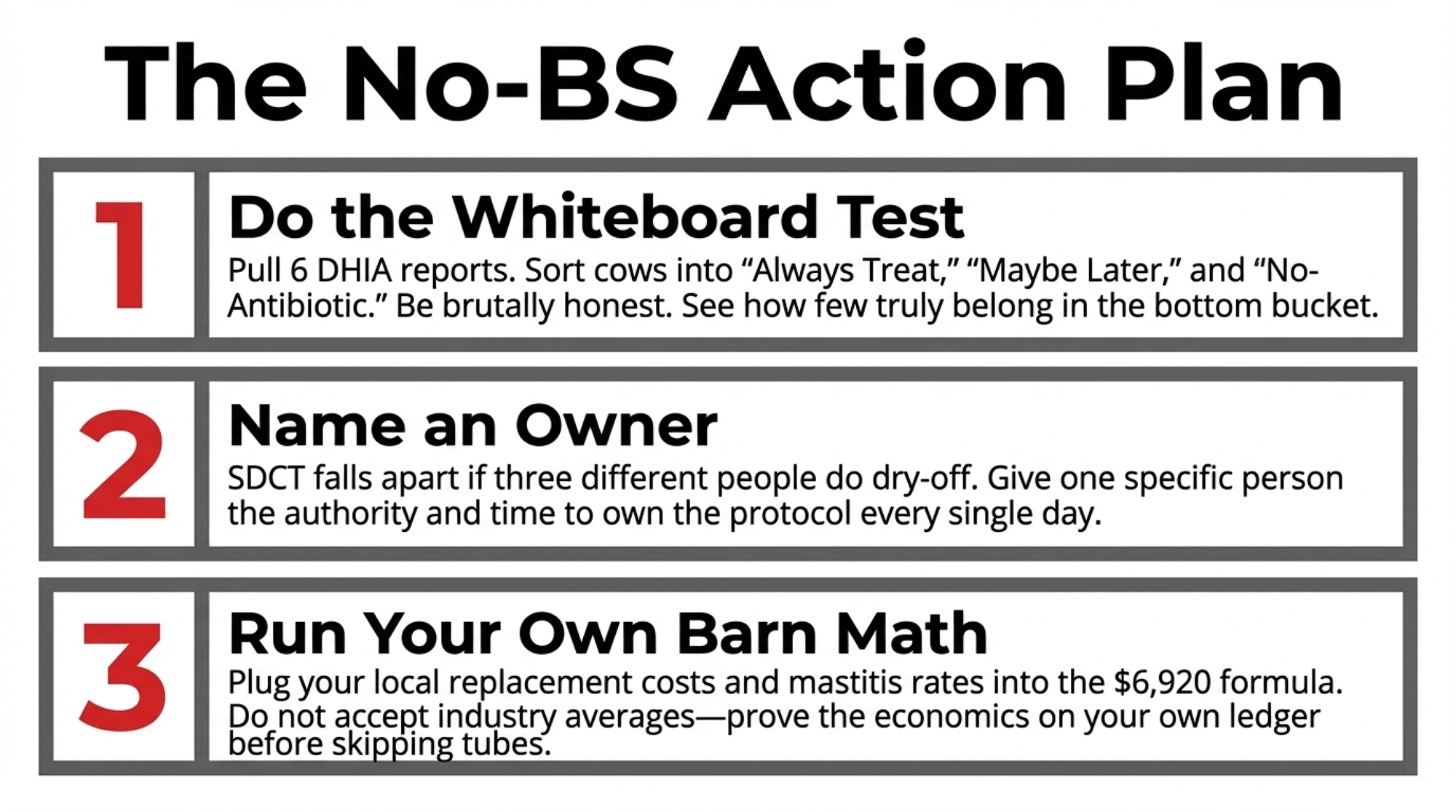
Do this within 30 days: Pull your last six DHIA reports and your current dry‑off list. On a whiteboard, make three columns:
- “Always treat”
- “Maybe selective later.”
- “Pilot no‑antibiotic candidate”
Fill it in honestly. That one exercise will show you how many cows truly belong in the lowest‑risk bucket — and how far your herd sits from one that looks like Mystic Valley or the Lipkens group.
3. Turn the Processor Letter Into Leverage, Not a Deadline
This fits herds that need time and capital to fix underlying issues while facing firm SDCT language from buyers.
Go back to the processor with a framework instead of a yes/no:
- You’ll pilot SDCT only on the safest slice (as in Path 2) this coming dry‑off season.
- You’ll report quarterly on the bulk tank SCC trend, the percentage of fresh cows with SCC over 200,000, and the first‑60‑day mastitis incidence.
- In return, you ask for a 12–18‑month runway to hit agreed improvements in SCC and mastitis, and to address facility bottlenecks, before any push toward wider SDCT.
The Dutch experience backs you up: that 47% dairy‑sector antimicrobial reduction happened over years, not months, and required simultaneous work on management, housing, and monitoring — not just a ban on tubes. A buyer who can show auditors your plan and your numbers is better off than one who forced SDCT onto a high‑SCC herd and then watched the metrics wobble.
What This Means for Your Operation
- Start with your own SCC curve, not the industry average. If your bulk tank has lived under 200,000 for the last 6–12 months and you can pull a trustworthy mastitis and SCC history for each cow, you’re in the same readiness zone as the Lipkens herds and Cornell’s average SDCT adopter. If you’re swinging 230,000–280,000, you’ve still got infection work ahead of you.
- Decide who owns dry‑off — by name. SDCT falls apart when three different people “kind of” handle it. One person needs to own that protocol and have enough time and authority to stick to it every day.
- Use the AABP checklist as your gatekeeper, not your processor’s email. Bulk tank SCC regularly less than 250,000; no Strep. ag; Staph. aureus under control; individual SCC data; written SOPs; sealant for all cows. If those boxes aren’t ticked, your herd is still in the infection‑reduction phase.
- Run your own barn math before you skip tubes. At a USDA average of $2,860 per replacement heifer — with individual animals clearing $4,000+ — even two extra early culls from mis‑classified SDCT cows can blow past a full year of tube savings. Put your own numbers into the $6,920 example; don’t just accept the model.
- Within 90 days: Sit down with your vet and put your last six months of SCC and mastitis data beside the AABP SDCT criteria. Wherever your herd fails on that checklist, that’s where your next management or capital dollar should go.
- Within 12 months: If you stay on BDCT while fixing management, re‑run your fresh‑cow SCC and first‑60‑day mastitis plots against last year’s. A noticeable step change does more to prove you’re SDCT‑ready than any pledge about tube counts.
Key Takeaways
- If your herd’s SCC isn’t consistently under ~200,000 and your records can’t reliably sort truly low‑risk dry cows from the rest, SDCT is a future objective, not a current target.
- If you pilot SDCT, every cow that skips tubes should have three consecutive SCC tests under 200,000, no mastitis this lactation, no problem quarters, and still receive a teat sealant — and you need to track her fresh‑cow outcomes separately from full‑treated cows.
- If fresh‑cow SCC or first‑60‑day mastitis in your SDCT group climbs above your own baseline, that’s your cue to pause or narrow and invest harder in infection control rather than hoping the numbers settle.
- If your processor is pushing a hard SDCT timeline, bring them a plan with a pilot cohort, monitoring metrics, and 12–18‑month milestones — not blanket SDCT on a 240,000‑SCC herd that isn’t structurally ready.
The Bottom Line
The herds that will be least stressed by the next round of antimicrobial stewardship rules aren’t the ones bragging about cutting the most tubes. They’re the ones whose data can prove their cows do fine without them.
When you pull up your last year of SCC curves, mastitis logs, and cull codes, do those numbers honestly look like a Mystic Valley‑style foundation for selective dry cow therapy — or are they telling you to keep the tubes while you fix what’s underneath?
Complete references and supporting documentation are available upon request by contacting the editorial team at editor@thebullvine.com.
Learn More
- Cut Mastitis Treatment Costs 60%: The $2.3 Billion Industry Secret That’s Reshaping Dairy Economics – Arms you with a diagnostic roadmap to slash discarded milk costs by up to 80%. This guide delivers the exact on-farm culture protocols needed to stop guessing on infections and start capturing immediate “Monday morning” savings.
- Stop Tightening Your Belt: Dairy’s $6.35/cwt Gap and Your 90-Day Window to Close It – Exposes the structural shifts in replacement heifer inventory and component pricing that will define your margins through 2028. It reveals how to reposition your herd to meet aggressive processor quality standards before the market decides for you.
- The Next Frontier: What’s Really Coming for Dairy Cattle Breeding (2025-2030) – Breaks down the emerging AI and sensor breakthroughs that detect mastitis a full week before clinical signs appear. It delivers a 5-year strategy to breed “invisible” cows that fundamentally outperform stewardship audits through superior natural immunity.
 The Sunday Read Dairy Professionals Don’t Skip.
The Sunday Read Dairy Professionals Don’t Skip.
 The Sunday Read Dairy Professionals Don’t Skip.
The Sunday Read Dairy Professionals Don’t Skip.Every week, thousands of producers, breeders, and industry insiders open Bullvine Weekly for genetics insights, market shifts, and profit strategies they won’t find anywhere else. One email. Five minutes. Smarter decisions all week.