Lose cows, save $277 on tubes, risk $2,220 in mastitis. Mystic Valley ran that math and still chose selective dry cow therapy. Would your herd?
Executive Summary: Mystic Valley Dairy tried selective dry cow therapy with all the “right” prerequisites—low SCC, Food Armor, strong records—and still lost cows in the first 60 days. Instead of reverting to blanket dry-cow therapy, they changed how they used teat sealant, tightened fresh‑cow monitoring, and kept SDCT in the protocol. This article pairs that real‑world experience with 2021–2024 research showing that algorithm‑guided SDCT can deliver average net returns of about 7–8 USD per cow at dry‑off and culture‑guided SDCT around 2 USD per cow, assuming udder health stays comparable to blanket therapy. It also draws on a 37‑herd Wisconsin cost study showing typical dry‑off product costs of about 19.57 USD per cow, with modeled SDCT protocols trimming partial direct costs by roughly 1–5 USD per cow, depending on product mix and how many cows still receive treatment. A simple barn‑math example for a 300‑cow herd (about 277 USD saved on tubes versus 2,220 USD in potential mastitis costs) turns SDCT from a philosophical debate into a concrete risk‑reward decision. Genetics aren’t an afterthought: health traits like mastitis resistance, livability, and DPR are positioned as the long‑term lever that makes SDCT safer and more scalable. The piece closes with a 90‑day playbook—paper‑testing an SDCT algorithm on last year’s dry‑offs, tightening records, and piloting one low‑risk group—plus clear “go/no‑go” signals on SCC, compliance, and mastitis trends so owners and herd managers can decide when SDCT makes sense and when it doesn’t.

In 2018, Mystic Valley Dairy in Sauk City, Wisconsin, was already an outlier — treating fewer than 20% of cows with antibiotics at dry‑off. Owner Mitch Breunig’s 450 registered Holsteins averaged just over 30,000 pounds of milk per cow, with a bulk tank somatic cell count sitting at 78,000 cells/mL. He’d already gone through the Food Armor antimicrobial stewardship program and was confident enough in his selective dry cow therapy (SDCT) system to change something most dairies still considered untouchable.
The results didn’t cooperate.
In published interviews, Breunig said the herd lost a couple of cows in the first 60 days of SDCT, likely due to toxic gram‑negative mastitis. He could’ve gone straight back to blanket dry cow therapy. Instead, he changed the way his team handled dry‑off — and doubled down on SDCT anyway.

Quick Stats: Mystic Valley and SDCT
- Herd: ~450 registered Holsteins, Sauk City, Wisconsin
- Milk: Just over 30,000 lb per cow per year (2018)
- Bulk tank SCC: ~78,000 cells/mL
- BAA: 105.2, ranked 7th in the U.S. for herds >300 cows at the time
- Dry‑off antibiotics: <20% of cows treated when SDCT began
- Energy‑corrected milk (2025): ~125 lb ECM/cow/day, 4.5% fat, 3.4% protein
Why Blanket Dry Cow Therapy Is Under Pressure
For decades, the default was simple: every cow, every quarter, every dry‑off got an antibiotic tube. Blanket dry cow therapy cured existing infections and helped prevent new ones during the dry period. It was effective and, honestly, easy.
That’s changing.

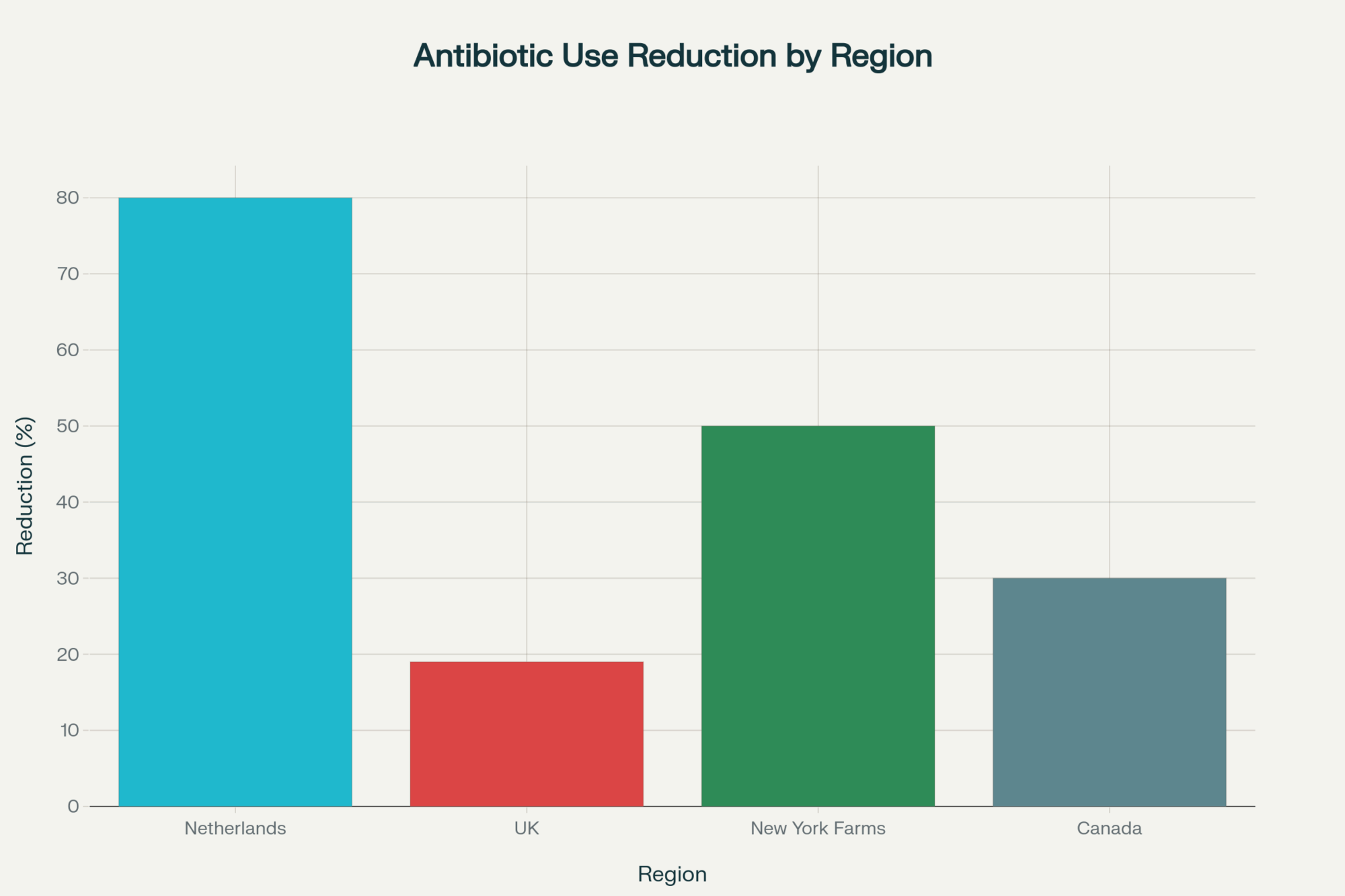
The EU’s Farm to Fork strategy targets a 50% reduction in antimicrobial sales for farmed animals and aquaculture by 2030, which directly pressures routine blanket treatments. In the U.S., the FDA’s Guidance for Industry #263 — which pulled all over‑the‑counter medically important antibiotics under veterinary oversight — took full effect in June 2023. In states like New York, lawmakers have introduced bills targeting routine or prophylactic antimicrobial use in food animals, adding another layer of scrutiny to practices such as blanket dry cow therapy.
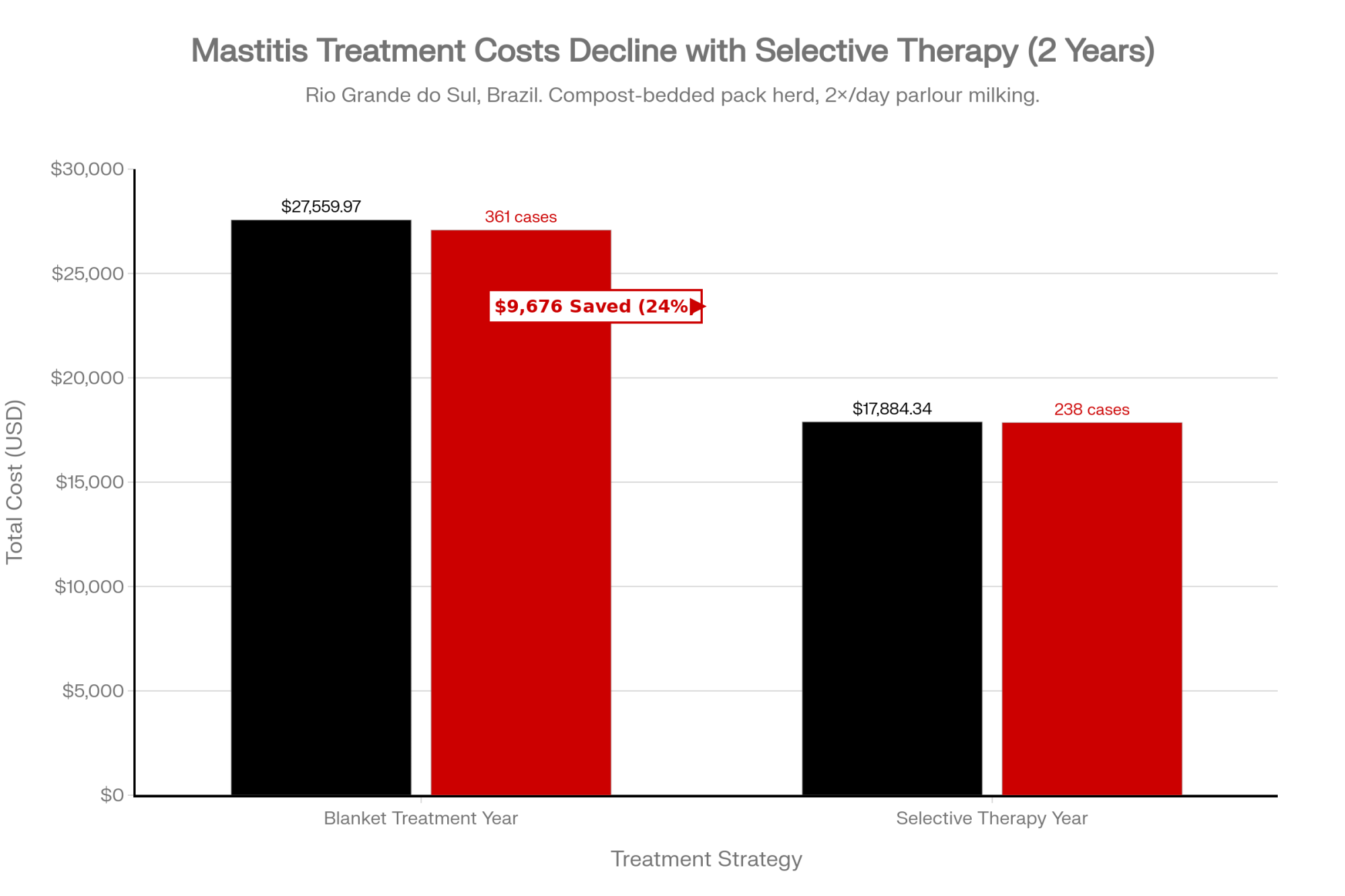
A Wisconsin study of 37 large herds found the average dry‑off product cost under blanket therapy was 19.57 USD per cow, with a range of 8.72–24.04 USD depending on the product mix. When researchers modeled a standard SDCT algorithm with fixed tube prices, the average modeled cost dropped from 18.68 USD per cow under blanket DCT to 17.69 USD per cow under SDCT, while observed farm‑specific antibiotic costs alone averaged 11.54 USD per dried cow (range 8.72–15.44 USD). There’s real spread between herds — and between products — in what dry‑off actually costs, which is why your per‑cow savings may land anywhere from “about a buck” to several dollars.
Not everyone thinks those dollars are a good enough reason to switch. Larry Fox at Washington State University has argued that there’s no solid evidence that blanket dry cow therapy has selected for resistant mastitis pathogens, and that, for many herds, the established protocol remains the safest default. That tension — between regulatory pressure, economics, and herd health reality — is exactly where selective dry cow therapy sits.
Algorithm vs. Culture: Two Selective Dry Cow Therapy Paths
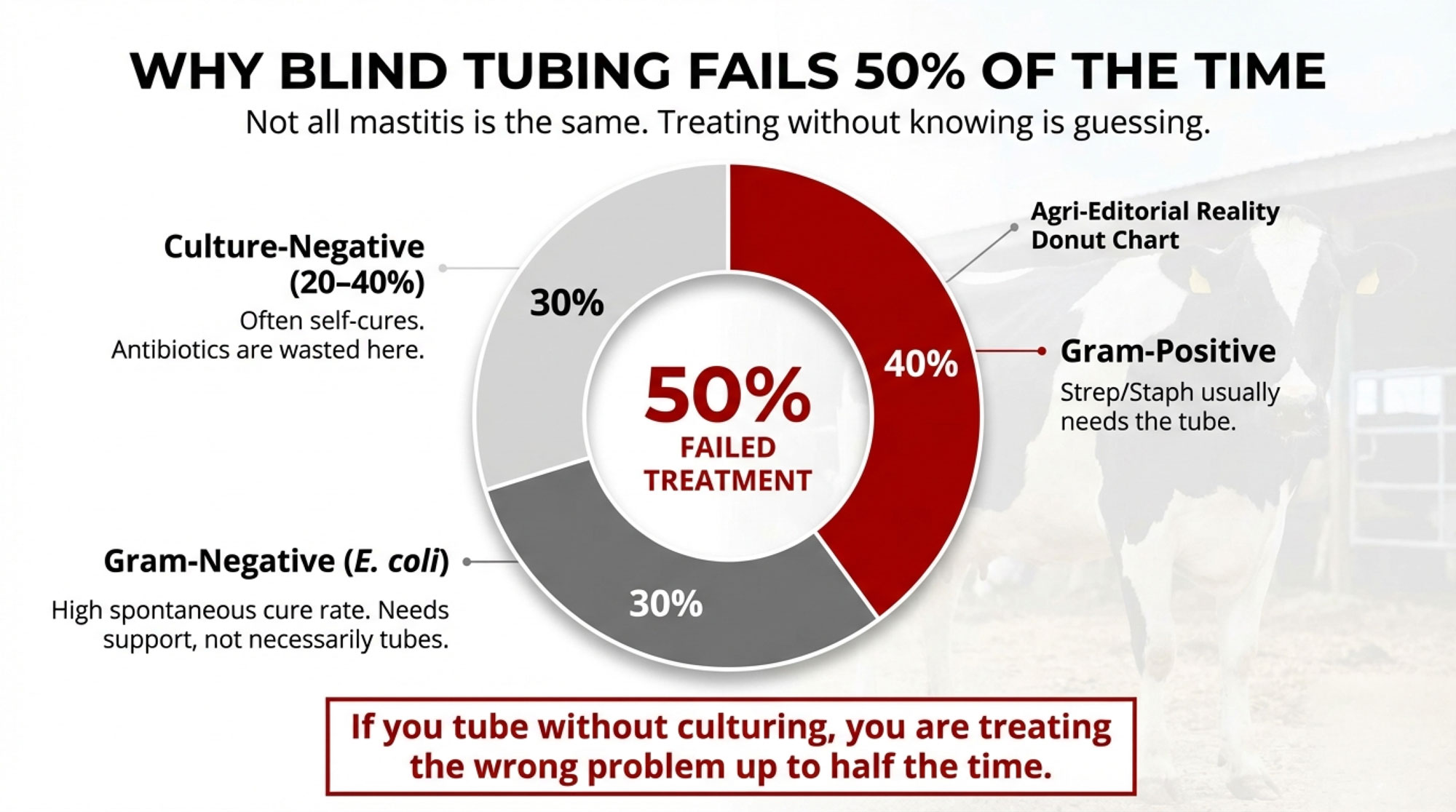
A lot of the SDCT debate boils down to how you decide who gets a tube.
Side‑by‑Side: Algorithm vs. Culture‑Guided SDCT

| Feature | Algorithm‑Guided SDCT | Culture‑Guided SDCT |
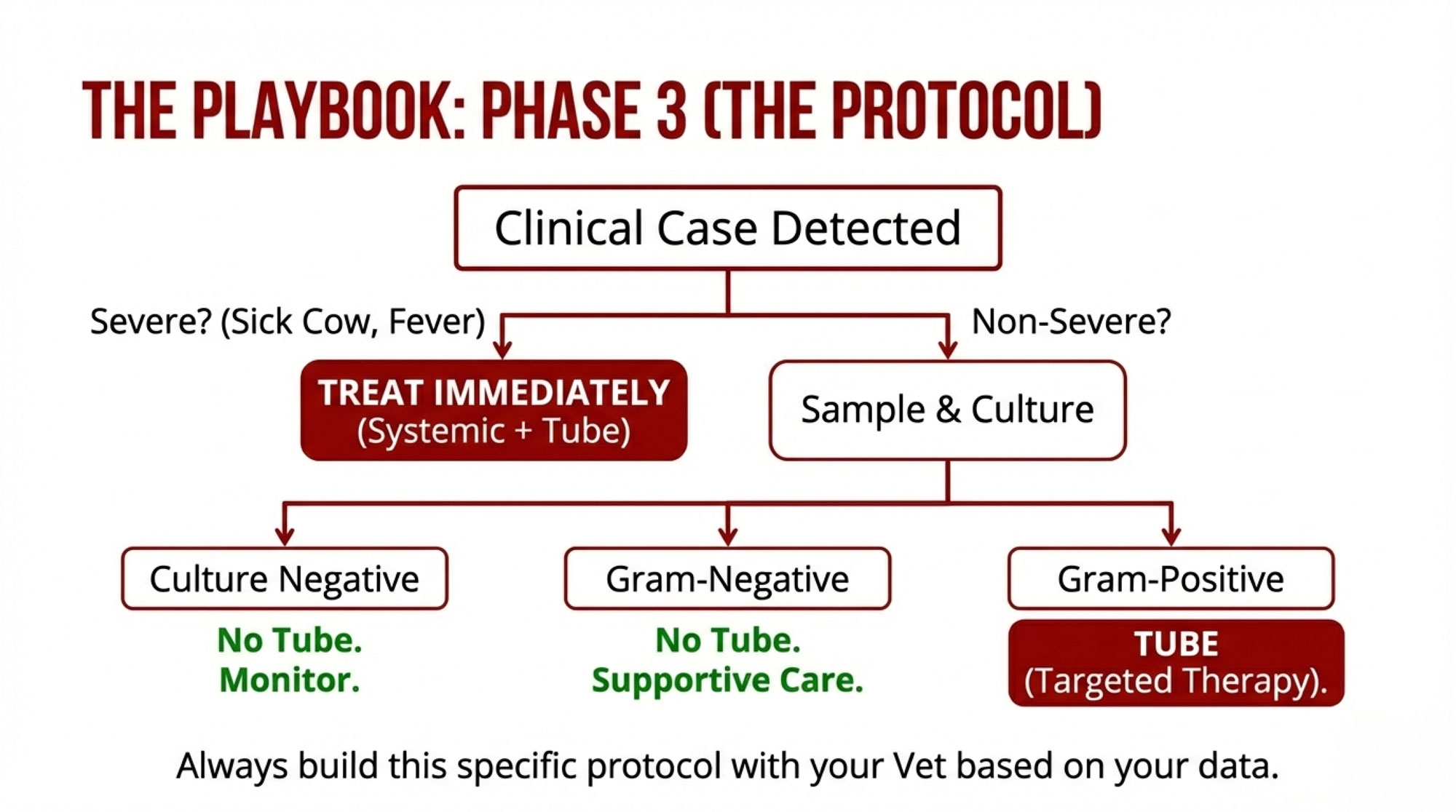
| Core input | DHIA SCC history, mastitis treatment records, sometimes milk at dry‑off | Quarter milk samples cultured before dry‑off on on‑farm media |
| Typical rule | Any SCC >200,000 cells/mL or clinical mastitis = antibiotic + sealant; others = sealant only | Treat based on what grows; high‑risk pathogens get antibiotic, low/no growth may get sealant only |
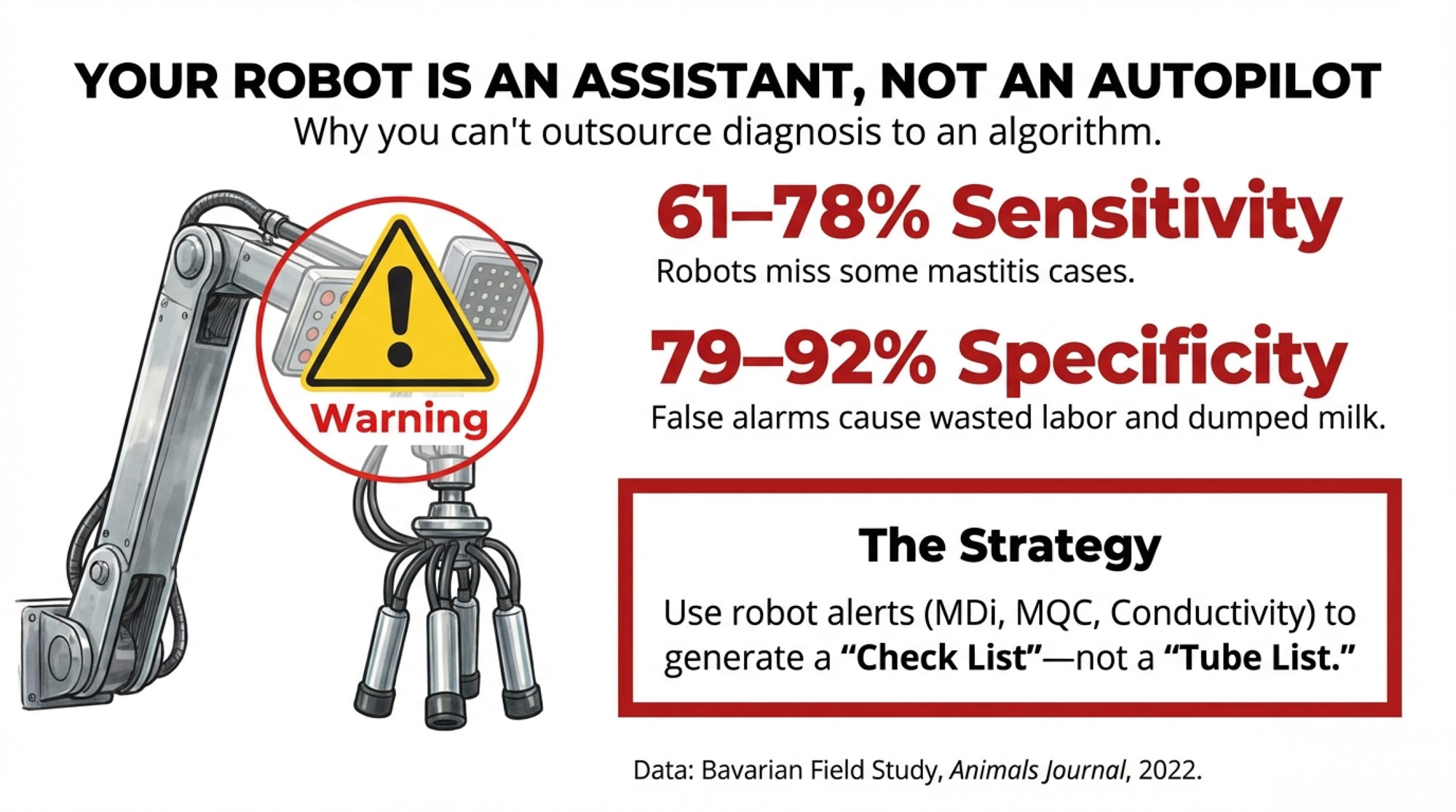
| Antibiotic reduction | Cuts dry‑off antibiotic use by roughly half in trial and field settings when protocols are followed | Similar magnitude of reduction when implemented correctly |
| Average economic impact | +7.85 USD per cow vs blanket (5–95%: 3.39–12.90 USD; 100% of iterations ≥0 USD) | +2.14 USD per cow vs blanket (range −2.31 to 7.23 USD; 75.5% of iterations ≥0 USD) |
| Strengths | Cheaper, faster, easy to implement where records are strong | More pathogen‑specific info that can improve mastitis control beyond dry‑off |
| Weak points | Relies heavily on SCC and mastitis records being accurate and complete | More labor, supplies, and training; practical fit for fewer herds |
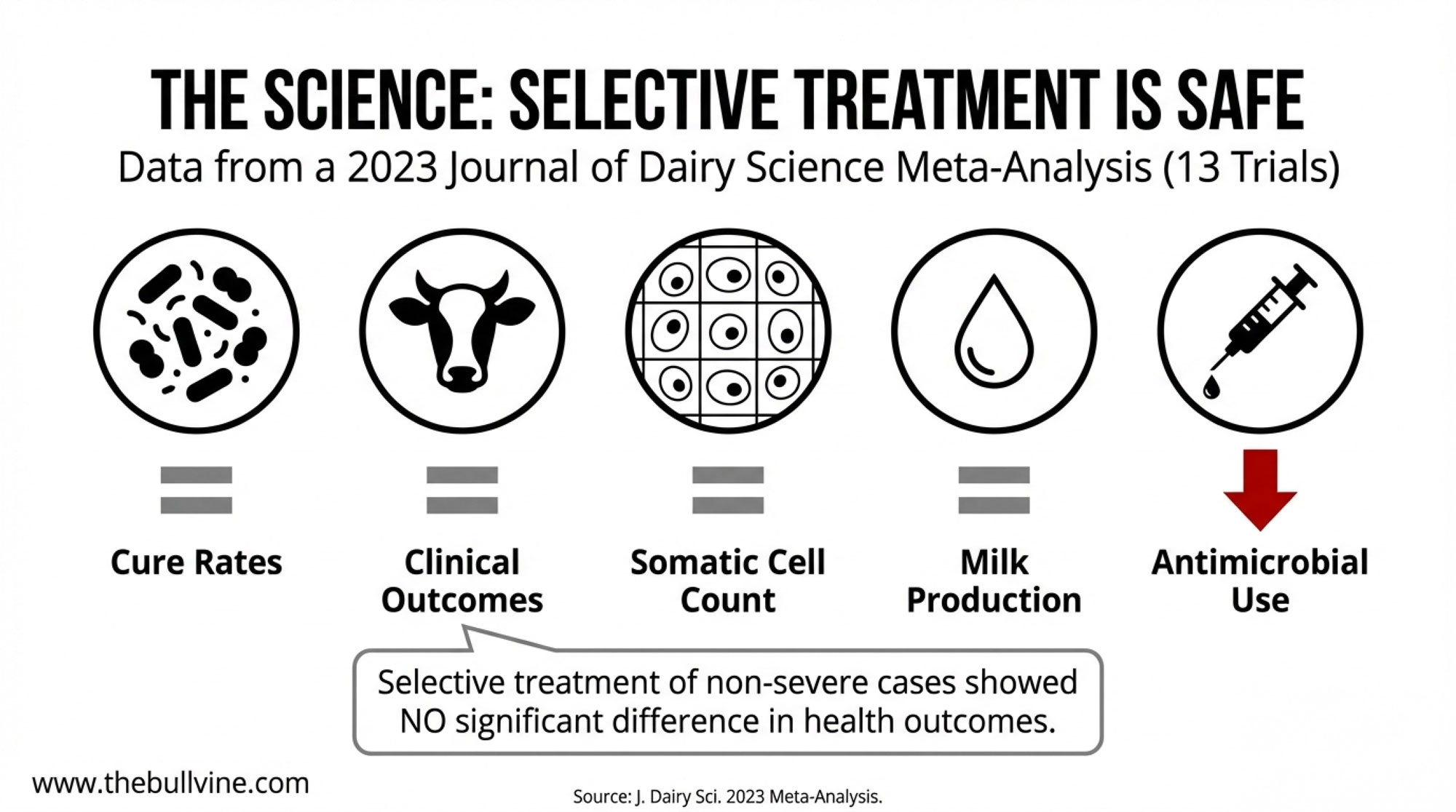
Rowe, Godden, Nydam, and colleagues’ 2021 partial budget analysis in the Journal of Dairy Science showed that when SDCT is implemented properly, both algorithm‑guided and culture‑guided programs can be economically favorable compared with blanket therapy, with algorithm‑guided SDCT delivering more consistent positive returns. The algorithm approach produced a mean net cash impact of +7.85 USD per cow, with every modeled scenario at or above break‑even, while culture‑guided SDCT averaged +2.14 USD per cow but included some scenarios with a small net loss.
In applied projects, including Cornell‑linked implementation efforts across New York dairies, farms tended to gravitate toward algorithm‑based SDCT because it fit better with their existing labor and record systems. Culture‑guided SDCT demanded more time, equipment, and training than many herds could justify. Health outcomes can be equivalent when the fundamentals are solid — but the logistics and risk tolerance aren’t the same across herds.
Inside Mystic Valley: The Criteria, the Crash, and the Turn
Breunig didn’t land on SDCT by accident. He came in through the Food Armor program, which forced his team to look hard at every antimicrobial they were using.
By 2018, his herd’s public record looked like this: 450 registered Holsteins, herd average just over 30,000 lb of milk per cow, bulk tank SCC around 78,000 cells/mL, and a BAA of 105.2, ranking the herd seventh in the U.S. for herds over 300 cows at the time. To decide which cows could skip antibiotics at dry‑off, he used four specific criteria: last SCC of the lactation, second‑to‑last SCC, peak SCC during the lactation, and any treatment for clinical mastitis. If any test was well above 200,000 cells/mL, or she’d been treated for mastitis, she still got antibiotic dry cow therapy; if not, she was a teat‑sealant‑only candidate.
On paper, that’s a textbook algorithm‑guided SDCT. The results didn’t match.

Breunig said the herd lost a couple of cows in the first 60 days, likely due to toxic gram‑negative mastitis. For any herd, losing cows in the first two months of a new protocol raises an immediate question: Is the system wrong, or the execution?
Breunig was initially using internal teat sealant on all cows — treated and untreated — at dry‑off. After those early losses, he changed course: Mystic Valley now uses internal teat sealant only on cows that also receive antibiotic dry cow treatment. That’s a departure from many published SDCT protocols, which typically recommend teat sealant on all cows, and it reflects Mystic Valley’s specific experience and veterinary guidance — not a one‑size‑fits‑all recipe.
He also tightened monitoring. The herd moved to weekly SCC checks at freshening to catch subclinical spikes before they became clinical mastitis or necessitated culling.
Over time, the system held. A later Bullvine profile reported Mystic Valley averaging about 125 pounds of energy‑corrected milk per cow per day with roughly 4.5% fat and 3.4% protein. Breunig has publicly attributed the progress to a lot of small management decisions lining up over time, and selective dry cow therapy was one of those decisions.
Can Your Records Actually Support This?

The science is the easy part. The messy part is your records.
Among 11 early‑adopter Italian dairy farms studied by Guadagnini, Moroni, and colleagues, a specific slice of SDCT non‑compliance emerged: 21% of cows that should have received antibiotic treatment at dry‑off were instead given only internal teat sealant. Those non‑compliant cows were 3.77 times more likely to have subclinical mastitis at their first DHI test post‑calving compared with cows that received the recommended antibiotic plus sealant.
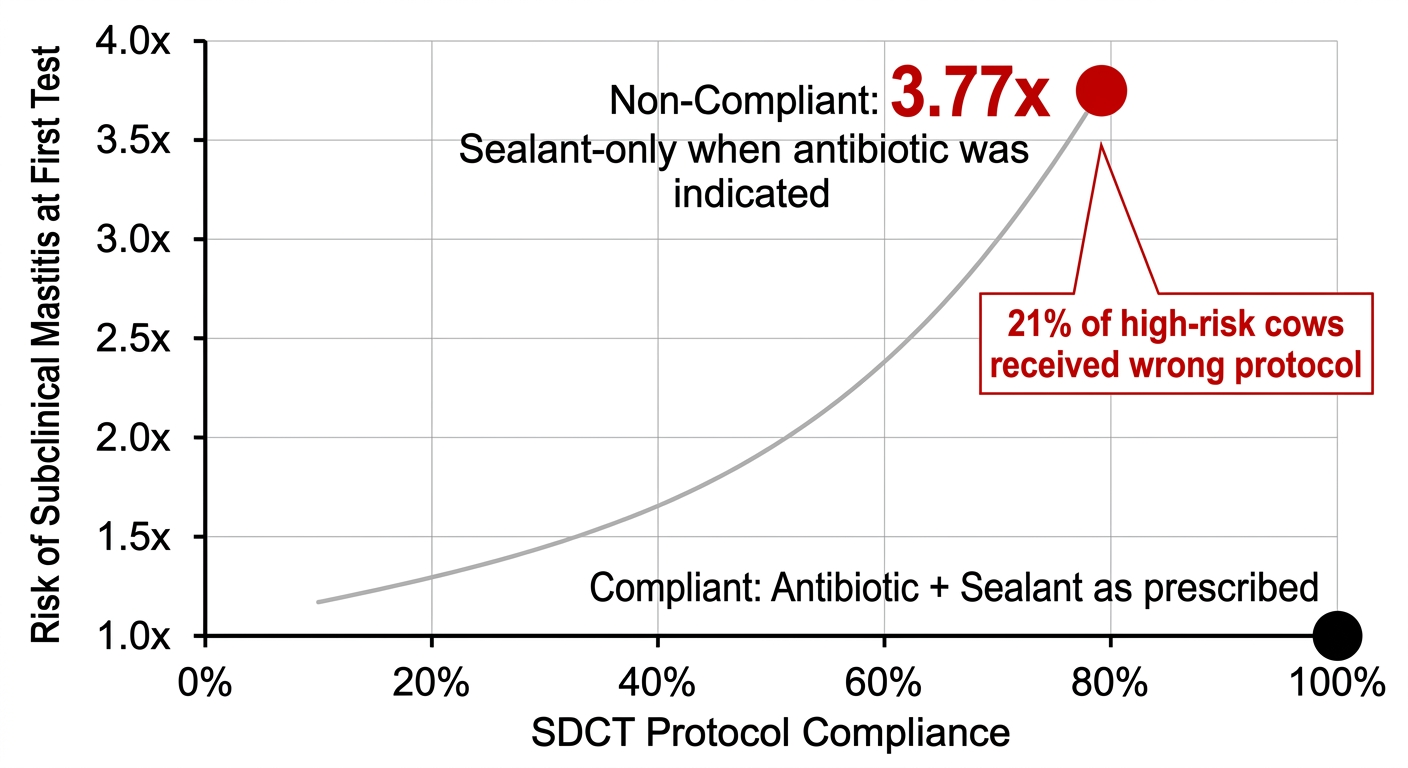
The research team reported that both veterinarians and farmers were unaware of the compliance deviation until data analysis was performed. When they dug into why it happened, 10 of the 11 herds attributed the problem to a lack of any monitoring system for whether the dry‑off protocol was actually being followed. There wasn’t malice or laziness. There just wasn’t a feedback loop, which is exactly how you end up with one in five high‑risk cows slipping through without the antibiotic the protocol calls for and a 3.77‑times higher risk of subclinical mastitis at first test.
A Cornell‑linked implementation project across New York dairies ran into the same kind of friction. The biggest barrier wasn’t herd health — it was recording and consistency. Some farms only started documenting mastitis events when they began SDCT, which made it look like mastitis was suddenly increasing when, in reality, they were finally writing everything down. A couple of herds pulled the plug on SDCT early, convinced it was causing extra mastitis in the dry period, and later review suggested that at least one of those spikes was part of a broader herd event unrelated to SDCT.
| Compliance Failure Point | What Happened in Research | Risk Multiplier | Fix Before You Start SDCT |
|---|---|---|---|
| No monitoring system | 10 of 11 Italian herds had no way to verify dry-off protocol was followed | 3.77x mastitis risk | Create dry-off checklist + weekly compliance audit |
| Incomplete mastitis records | NY herds only started logging clinical events when SDCT began; looked like spike | False alarm, protocol pause | Backfill 12 months of mastitis/treatment history |
| Crew turnover/training gaps | High-risk cows received sealant-only when algorithm called for antibiotic | 21% non-compliance rate | Written protocol + hands-on demo for every person doing dry-off |
| Seasonal pressure ignored | Some herds ran SDCT through peak heat; environmental mastitis spiked | Not quantified, but protocol paused | Pilot SDCT in lowest-risk season (fall/winter in most climates) |
| Blame the wrong variable | Herds attributed mastitis increases to SDCT when broader herd event was occurring | Early protocol abandonment | Track 0–90 DIM mastitis separately; compare to baseline by dry-off group |
Then there’s Jean Amundson — a veterinarian and co‑owner of Five Star Dairy near Elk Mound, Wisconsin. She and her partners milk about 1,000 cows and ship around 90 pounds of milk per cow per day. Amundson enrolled her herd in a University of Minnesota SDCT research trial and reported that the trial reduced dry‑cow antibiotic use by about half, thereby validating their approach. But her herd had been running on‑farm cultures and tight treatment records for years before the trial; selective dry cow therapy didn’t strengthen their data, strong data made SDCT possible.
The Genetics Angle: Why Health Traits Matter for SDCT
SDCT lives at the intersection of management and genetics.

The Council on Dairy Cattle Breeding (CDCB) publishes a mastitis resistance evaluation (MAST PTA) expressed as percentage points above or below the breed average, and these evaluations are favorably correlated with lower somatic cell scores, longer productive life, and better livability and fertility. That matters for SDCT because the herds that do best with selective dry‑off are the ones with consistently low SCC, good cure rates, and fewer chronic cows — exactly the profile you build when you lean harder on mastitis resistance and health traits in sire selection.
As you put more selection pressure on health traits — including mastitis resistance, livability, and fertility — in your breeding program, you’re gradually building a herd with fewer high‑risk animals at dry‑off and more cows that legitimately qualify as “low risk” in an SDCT algorithm. Over time, that shrinks the gap between what the algorithm recommends and what you’re actually comfortable doing.
The published SDCT studies in Italy, Belgium, and North America mostly focus on protocols, economics, and compliance rather than dissecting the role of genetic evaluations in those herds. But the direction is clear: genetics and management are beginning to work together to address mastitis, and herds that lean into both will have more room to pull tubes without paying for it in the fresh pen.
Does the SDCT Math Actually Pencil Out on Your Farm?
So what does the math look like when you actually take the tubes out of the cart?
Leite de Campos and Ruegg’s 37‑herd Wisconsin study provides a real‑world benchmark for direct product costs, assuming udder health remains comparable between blanket DCT and SDCT. That’s the starting point before you ask what happens if mastitis creeps up:

- Average blanket‑therapy dry‑off cost (observed): 19.57 USD per cow (range 8.72–24.04 USD)
- Average cost per dried cow when only intramammary antibiotic DCT was considered: 11.54 USD, with a range from 8.72 to 15.44 USD across herds
- Modeled cost using fixed prices for intramammary products: 18.68 USD per cow for blanket DCT vs 17.69 USD per cow for selective DCT — about 0.99 USD per cow savings at those standard prices
Other modeled scenarios in that dataset and related work show that, depending on product choices and how aggressively you pull tubes, partial direct cost reductions can reach roughly 5 USD per dry cow in some herds, but be closer to 1 USD in others. The per‑cow savings on tubes can range from “a noticeable line item” to “pretty modest,” depending on your current products and how aggressively you already use them.

If you’re running a 300‑cow herd and drying off about 280 cows a year, a 0.99 USD per‑cow savings at dry‑off is roughly:
280 cows × 0.99 USD ≈ = 277 USD in tube savings per year at standardized prices.

If your current protocol uses higher‑priced tubes and extensive sealant, your actual product savings under SDCT could exceed the modeled figure; if you already run a lean protocol, your savings could be smaller.
Year one is messier. You’ll spend money and time on veterinary consults to set up a herd‑specific algorithm, cleaning up mastitis and SCC records, writing a protocol people can actually follow at 4:30 p.m. in the parlor, and training the crew that does the dry‑off work. There isn’t a clean, published “X USD per herd” setup figure for this, but you should plan on meaningful first‑year overhead in vet time, staff time, and management attention that might eat most of the savings in year one.

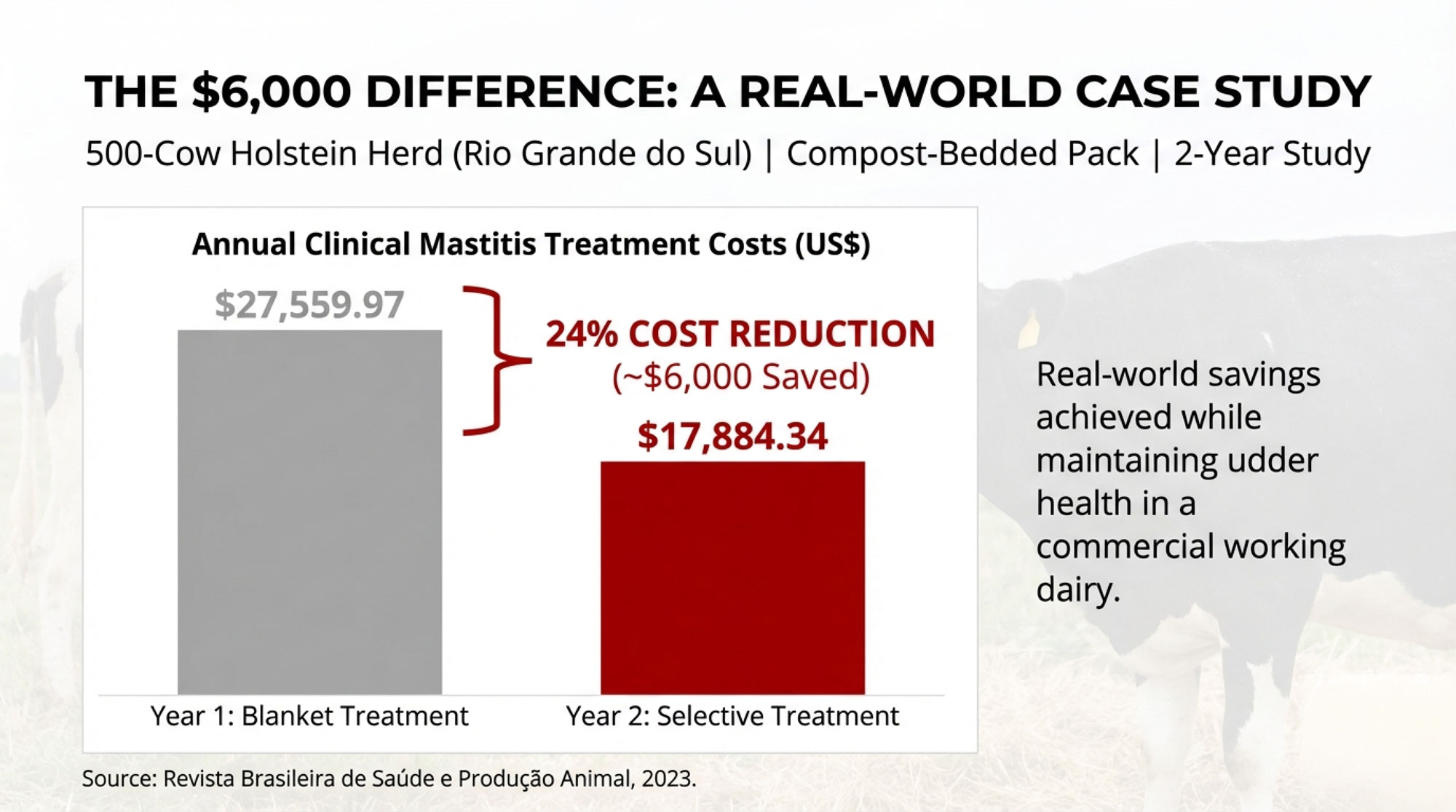
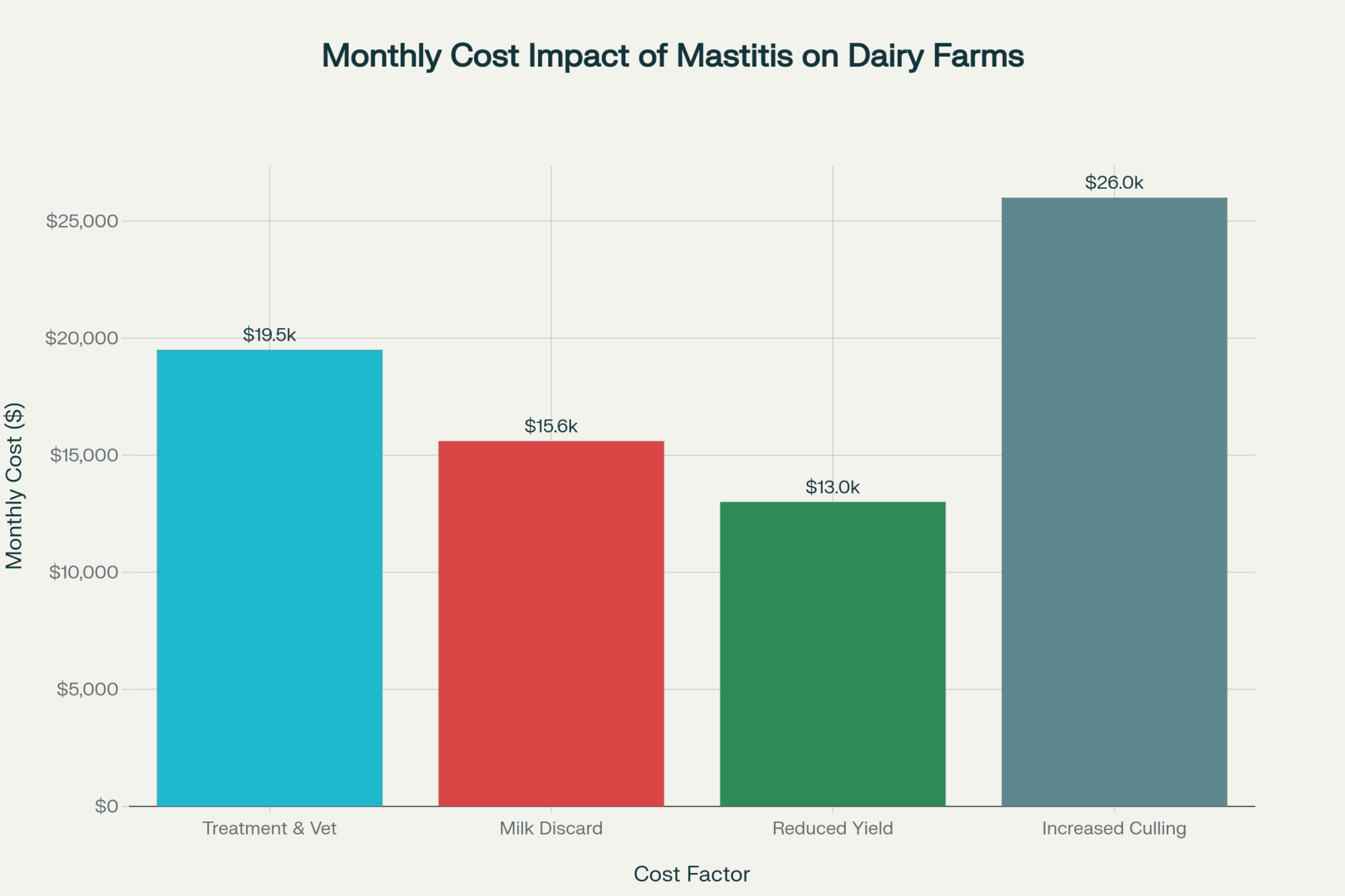
And if your execution is sloppy, it can eat more than that. Rollin and colleagues estimated the total economic cost of a clinical mastitis case in the first 30 days of lactation at approximately 444 USD per case on U.S. dairy farms, including direct costs and lost future milk. Turn five extra fresh‑cow mastitis cases loose because you misclassified cows or botched dry‑off hygiene, and you’ve just burned 5 × 444 USD = 2,220 USD — easily more than a year’s worth of SDCT tube savings for a 300‑cow herd under many product‑cost scenarios.
Your quick math: take the number of cows you dry off per year and multiply by a realistic, herd‑specific per‑cow savings number — which might be around 1 USD per cow if your current drugs and sealant use look like the modeled Wisconsin herds, and potentially more if you’re using higher‑priced tubes. Then set that against the cost of a handful of extra mastitis cases at roughly 444 USD each.
Now ask yourself what one bad dry‑off month — with a half‑dozen explosive mastitis cases — would do to that balance.
What This Means for Your Operation
These aren’t talking points. They’re checks you can run on your own herd.
- Can you pull a complete SCC and mastitis treatment history for every cow in your current lactation? If the answer is “sort of” or “not really,” SDCT should wait; your first 30 days should go into fixing the records, not the tubes.
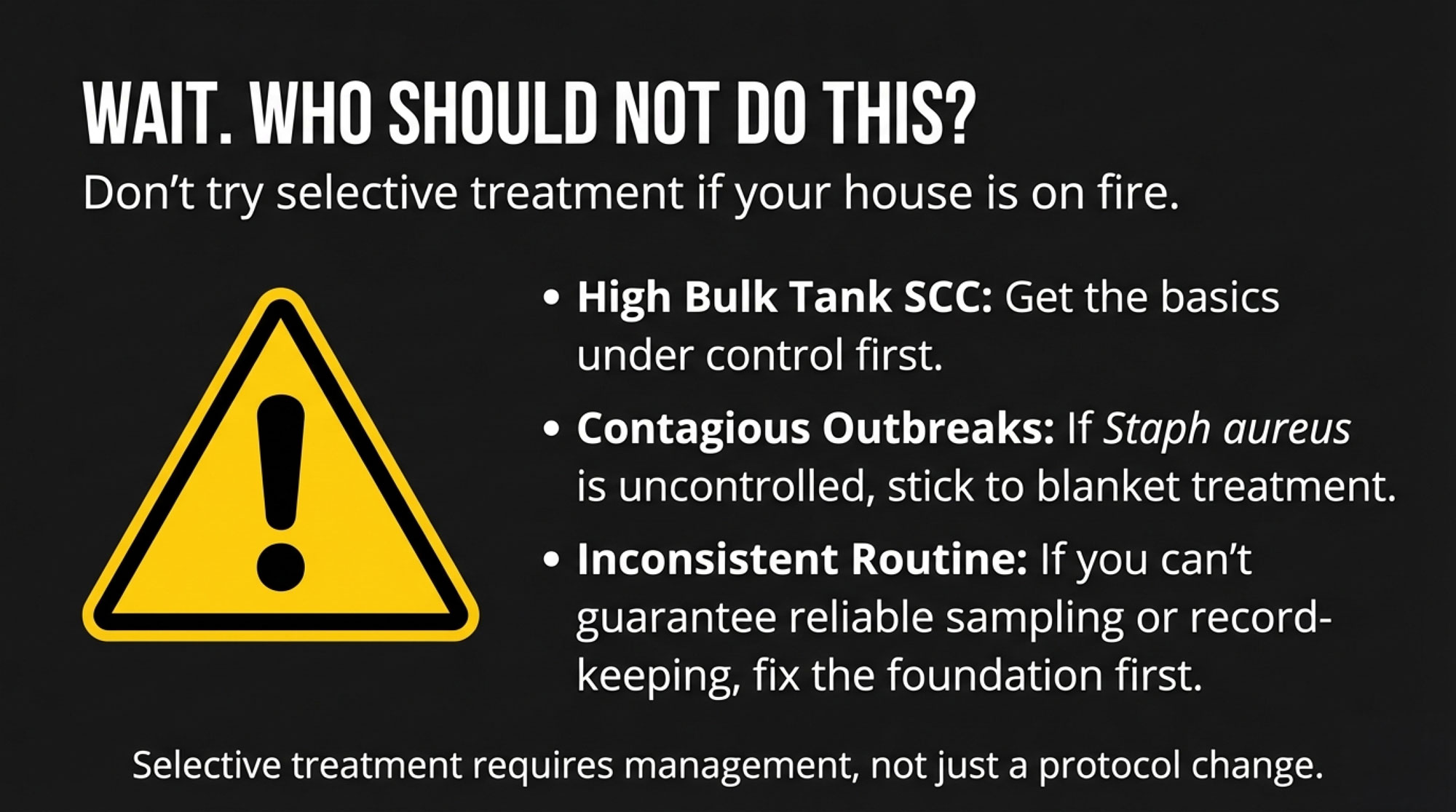
- Do you know your pathogen mix? At minimum, confirm your herd is clear of Streptococcus agalactiae and has Staphylococcus aureus under control before you pull antibiotics at dry‑off, because SDCT is a bad place to discover a chronic contagious mastitis problem.
- Who actually does dry‑off on your farm? The more people involved, the more ways the protocol can drift, and European work on dry‑off routines and the Cornell experience both found that technique — not theory — was often the weak link, which is why checklists and monitoring systems matter.
- Is your dry pen ready for cows without antibiotic safety nets? Stocking density, bedding, ventilation, and transition management all matter more when more quarters head into the dry period with only a teat sealant barrier.
- When would you start? Some New York herds in that implementation work paused SDCT during peak heat when environmental mastitis pressure spiked; if you’re going to experiment, start in your lowest‑risk season.
- Are you tracking fresh‑cow mastitis separately? If your 0–90 DIM mastitis rate climbs more than about two percentage points above your pre‑SDCT baseline for two consecutive dry‑off groups, that’s a loud signal to pause and audit before continuing.
- Can your software help? Herd software like DairyComp 305 and others can run SDCT‑style classifications off DHIA data or at least help you pull the logic together in reports; if you’re not on a full‑featured platform, even a simple spreadsheet with cow IDs, SCC history, and mastitis events can get you close as long as the data’s real.
- Is your breeding program moving in the right direction? If you’re already pushing health traits tied to mastitis resistance and cow longevity in your AI matings — including CDCB mastitis resistance, livability, and DPR where available — you’re quietly building a herd that should be a better SDCT candidate five years from now than it is today.
- Where do you want to be in a year? Within 12 months of your first pilot, you should be able to decide — based on your own mastitis and SCC data — whether SDCT is a permanent protocol, a seasonal tool, or something you park for now.
What to Do in the Next 90 Days
You don’t need to change a tube or buy a culture plate to learn something useful.
First 30 days
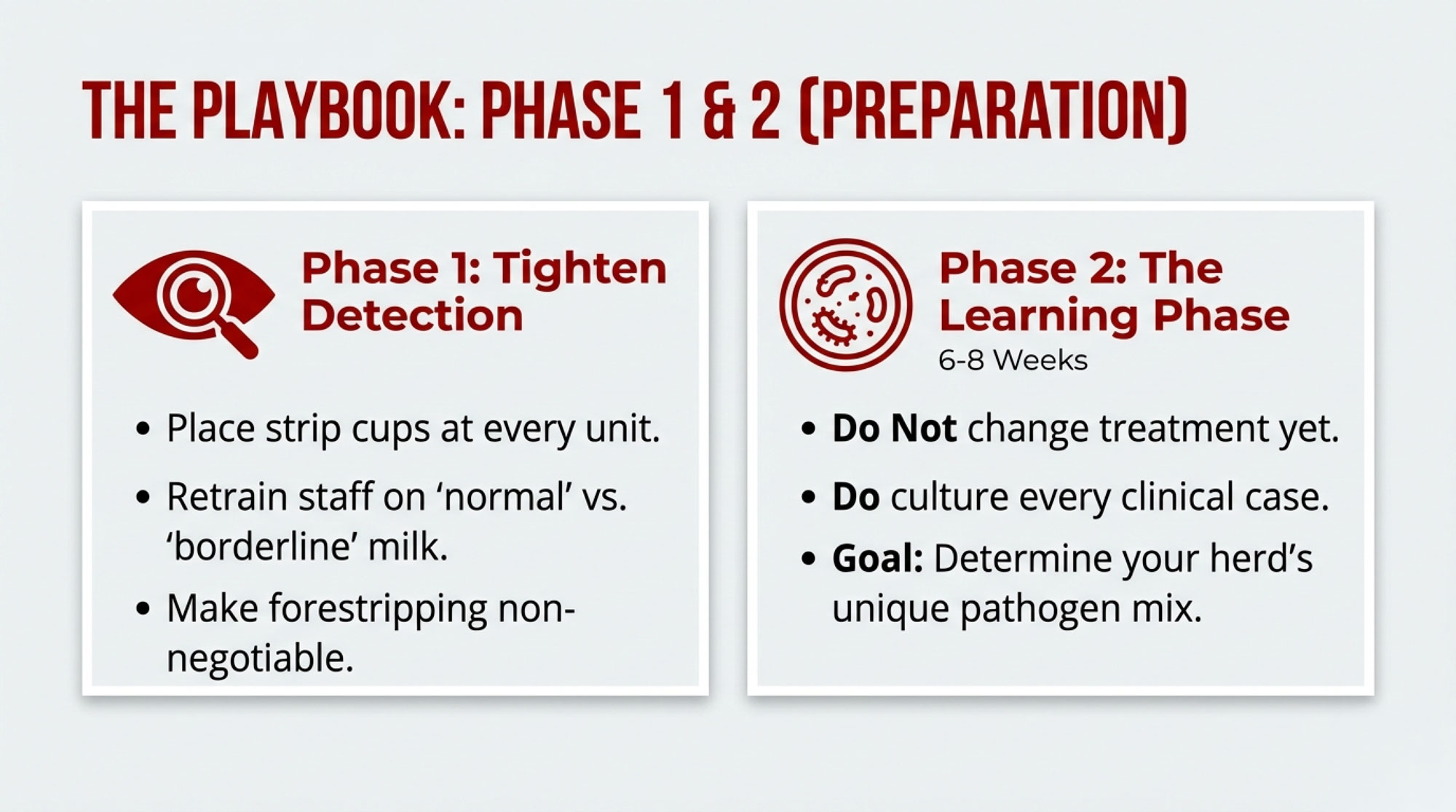
- Pull your last 12 months of DHIA records and export the SCC history for every cow you dried off in that period.
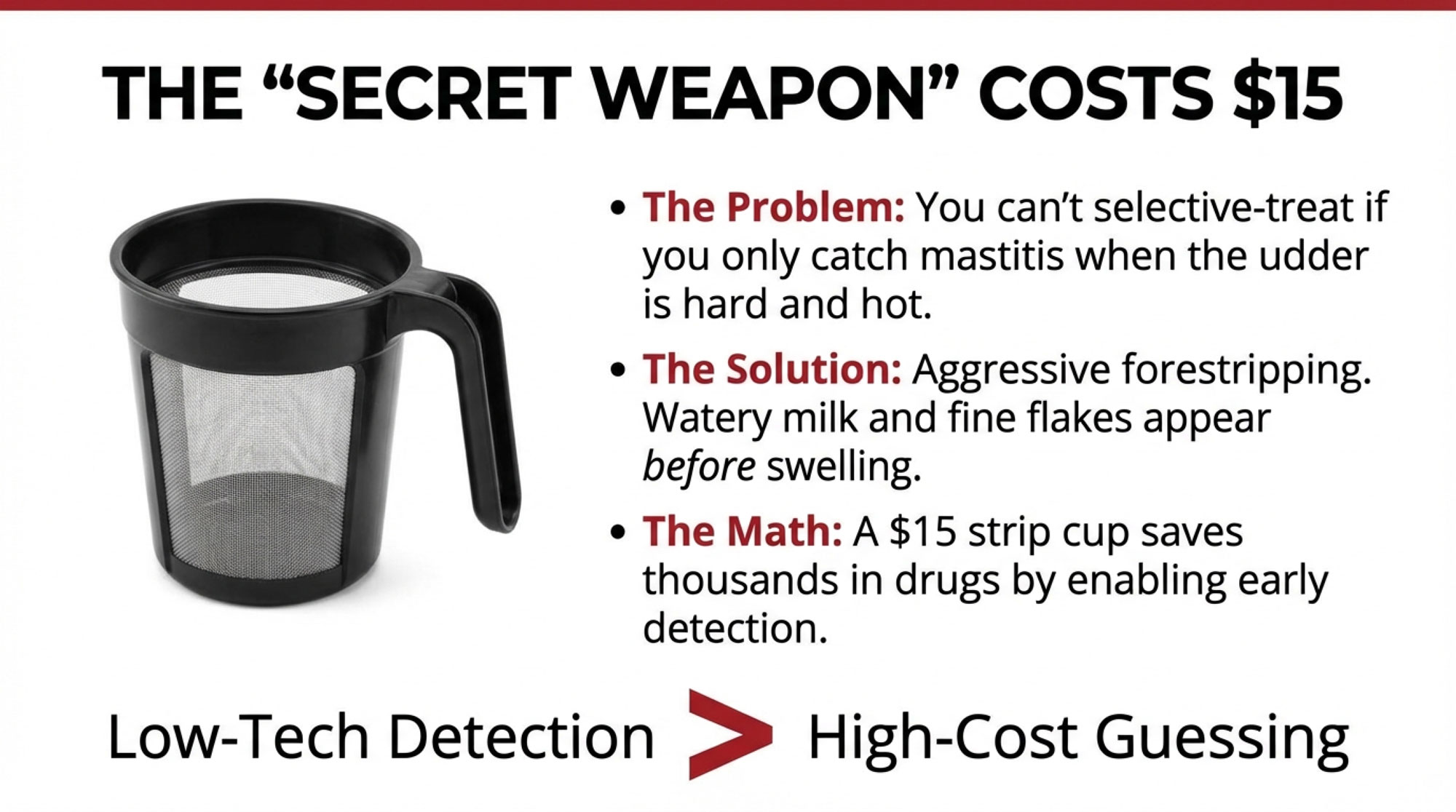
- Run a simple SDCT algorithm on paper: for each dry‑off, ask “Did this cow ever test over 200,000 SCC this lactation, or receive clinical treatment for mastitis?” and mark which cows would’ve been “sealant‑only.”
- Compare your “sealant‑only” list to fresh‑cow outcomes: which of those cows had mastitis in the first 30 days of lactation, and which ones were clean all the way through?
If that paper exercise makes you sweat, that’s useful information; it shows you where your protocol or your confidence is weak before you risk the cows.
Days 30–90
- Sit down with your vet and walk through the results from the paper exercise: where do your records have gaps, where does the algorithm agree with what you already suspected, and where does it surprise you?
- If the paper exercise looked promising, pilot SDCT on one dry‑off group during your lowest environmental mastitis pressure window, monitor 0–90 DIM outcomes for that group against your baseline, and track compliance from day one.
- At the same time, pull your last two proof runs and look at how strongly you’re actually selecting for health traits tied to mastitis risk and longevity — including mastitis resistance and related CDCB health traits where available — and adjust your mating plan before you treat SDCT as your new normal if those traits are an afterthought.

Key Takeaways
- If your bulk tank SCC isn’t consistently under about 250,000 cells/mL, your mastitis records aren’t rock solid, or you haven’t cleaned up contagious pathogens like Strep agalactiae and Staph aureus, SDCT isn’t your next move; tighten those fundamentals and fix the bugs first.
- Algorithm‑guided SDCT can deliver savings on tubes — but the per‑cow number is often modest, and the real money is made or lost in mastitis cases, not boxes of product; a few extra fresh‑cow mastitis cases can easily erase a year’s worth of tube savings.
- Compliance isn’t a detail, it’s the whole ballgame: those Italian early‑adopter herds saw one in five high‑risk cows miss the antibiotic they should’ve received, and those cows were 3.77 times more likely to show up with subclinical mastitis at first test.
- Genetic selection for health traits is now real and measurable: CDCB health traits — including mastitis resistance — and their favorable correlations with somatic cell score, productive life, and fertility give you a way to breed cows that fit SDCT better over time instead of relying on management alone.
- The safest way to start is on paper: running the algorithm on last year’s dry‑offs gives you a real‑world stress test of your data and your cows’ behavior without risking this year’s dry pen.
The Bottom Line
Mystic Valley’s first 60 days on SDCT included cow losses that would’ve sent most herds back to blanket therapy, but Breunig changed his sealant protocol, tightened monitoring, and kept going. Amundson’s herd at Five Star Dairy got there after years of building a culture‑and‑records foundation, and the University of Minnesota trial basically confirmed they were on the right track.
The tubes you pull — or don’t — on your farm will sit on top of your own system, not theirs. If your system can’t spit out clean mastitis data and your dry‑off crew can’t follow a checklist on a busy Friday, pulling tubes is the wrong place to start. So before you put down the dry cow gun, here’s the real question: if you ran a selective dry cow therapy algorithm on your last 100 dry‑offs tomorrow, would you trust what it told you?
Complete references and supporting documentation are available upon request by contacting the editorial team at editor@thebullvine.com.
Learn More
- 83% of Dairies Overtreat Mastitis – That’s $6,500/Year Walking Out the Door – Slash unnecessary expensesby mastering on-farm culture systems. This breakdown reveals the $6,500 error most herds make and arms you with a 90-day protocol to reclaim lost margins through precision treatment and smarter culling.
- Dairy Profit Squeeze 2025: Why Your Margins Are About to Collapse (And What to Do About It) – Position your operation to survive the 2025 margin collapse. This strategic roadmap exposes the ‘Margin Mirage’ and delivers four non-negotiable risk management actions to shield your balance sheet as All-Milk prices erode and feed costs fluctuate.
- The Next Frontier: What’s Really Coming for Dairy Cattle Breeding (2025-2030) – Unlock the biological advantage hiding in your breeding program. This look at the 2025–2030 frontier breaks down how new health-trait markers for mastitis resistance and genomic testing will fundamentally replace traditional “treat-and-wait” management strategies.
 The Sunday Read Dairy Professionals Don’t Skip.
The Sunday Read Dairy Professionals Don’t Skip.
 The Sunday Read Dairy Professionals Don’t Skip.
The Sunday Read Dairy Professionals Don’t Skip.Every week, thousands of producers, breeders, and industry insiders open Bullvine Weekly for genetics insights, market shifts, and profit strategies they won’t find anywhere else. One email. Five minutes. Smarter decisions all week.