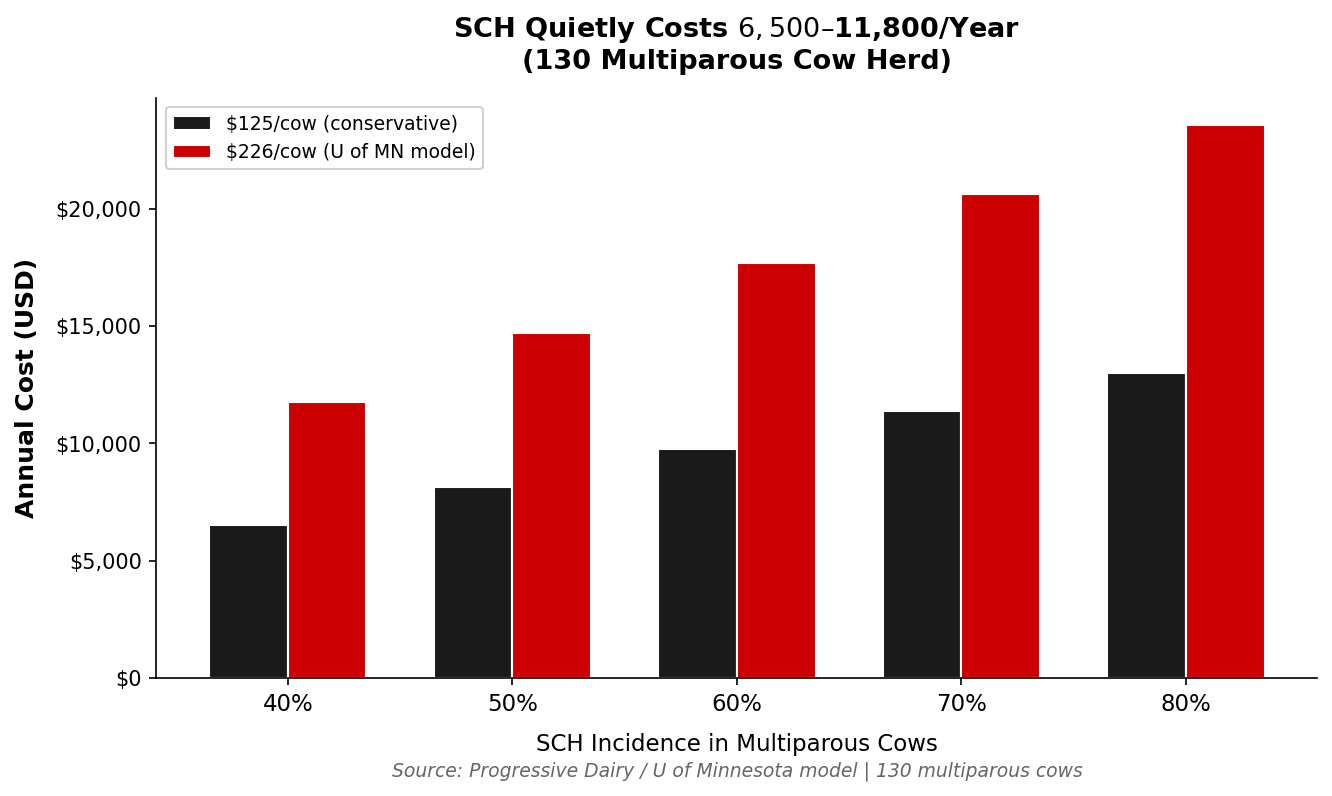
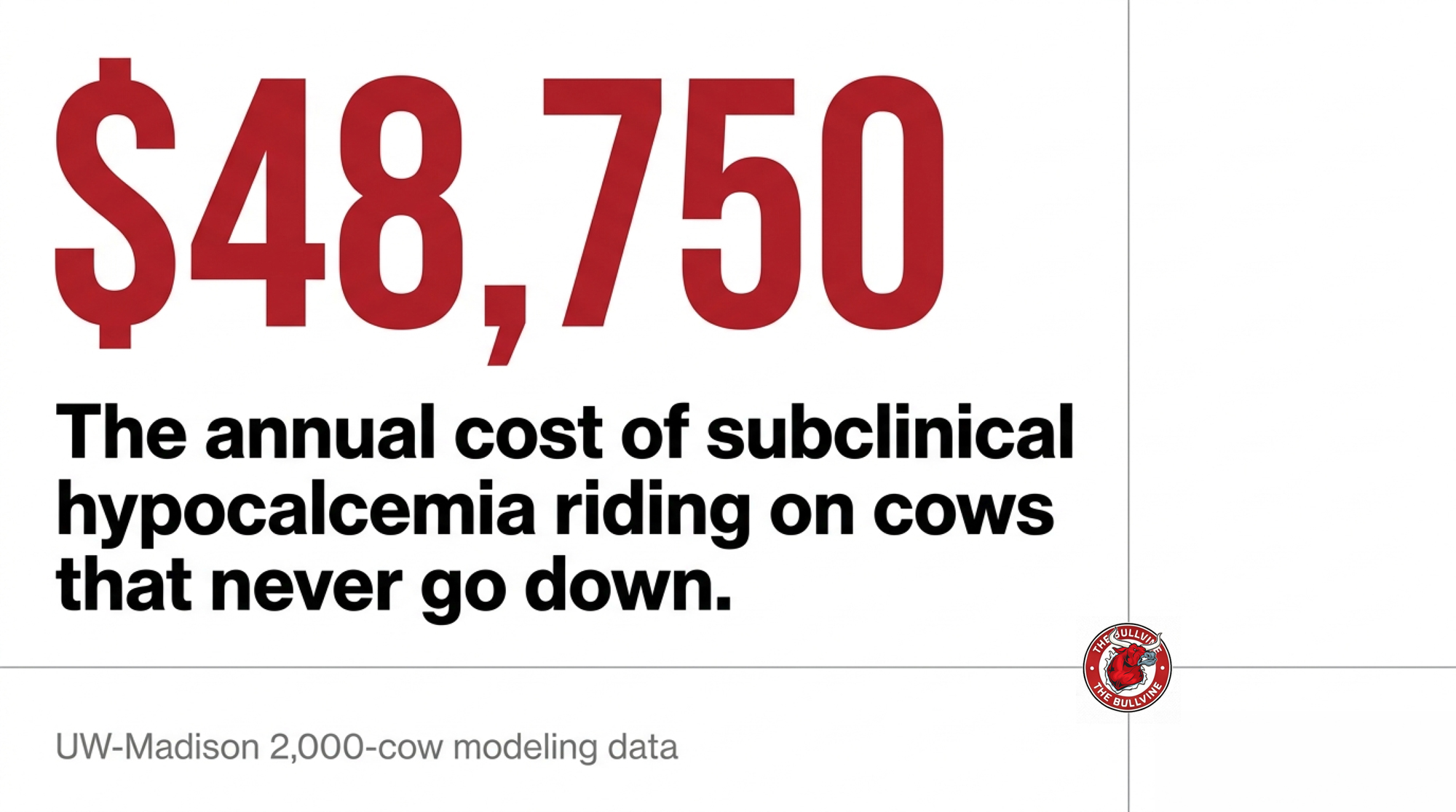
Your milk fever rate looks great. The $48,750 you’re losing on day-4 calcium never shows on that board — and it’s riding on cows that never went down.
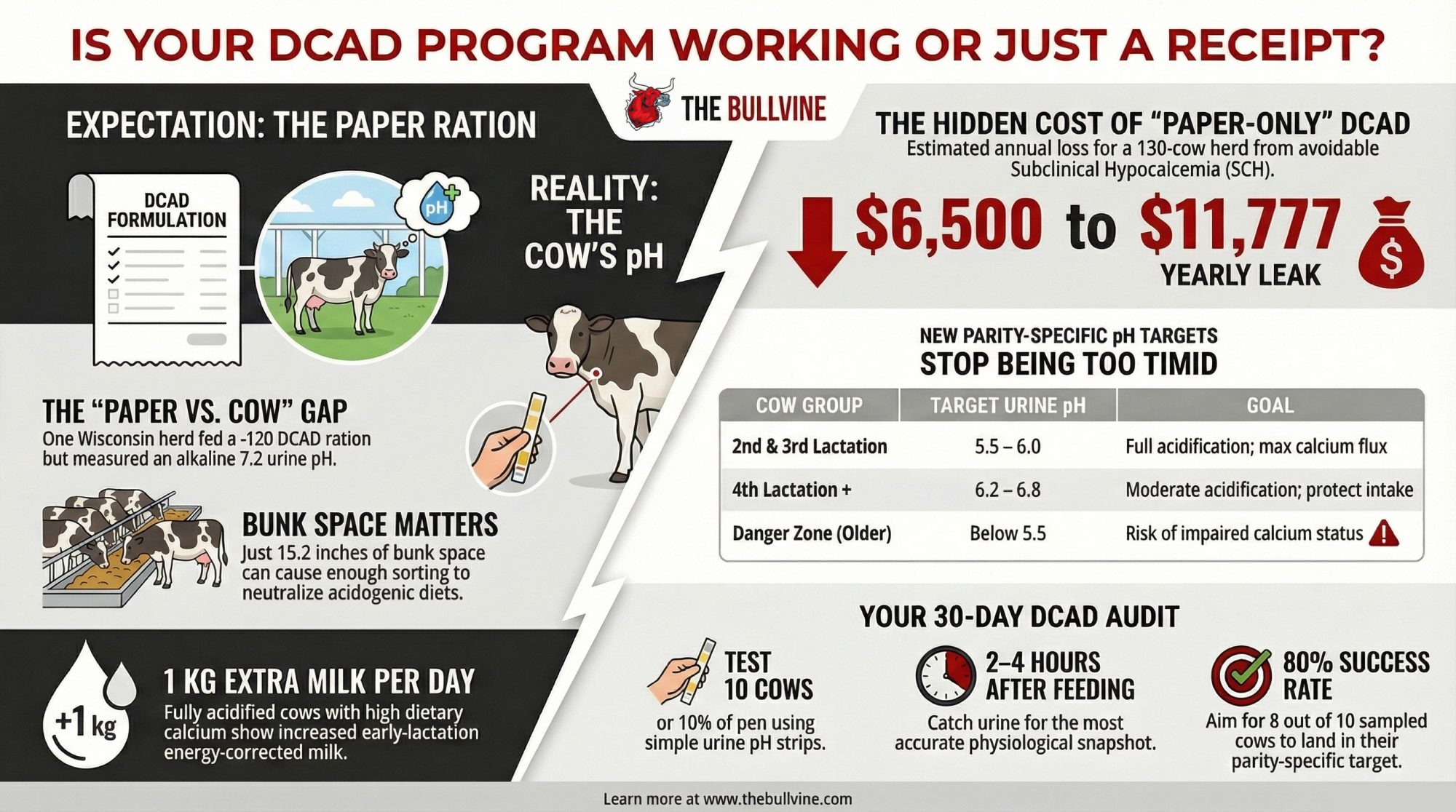
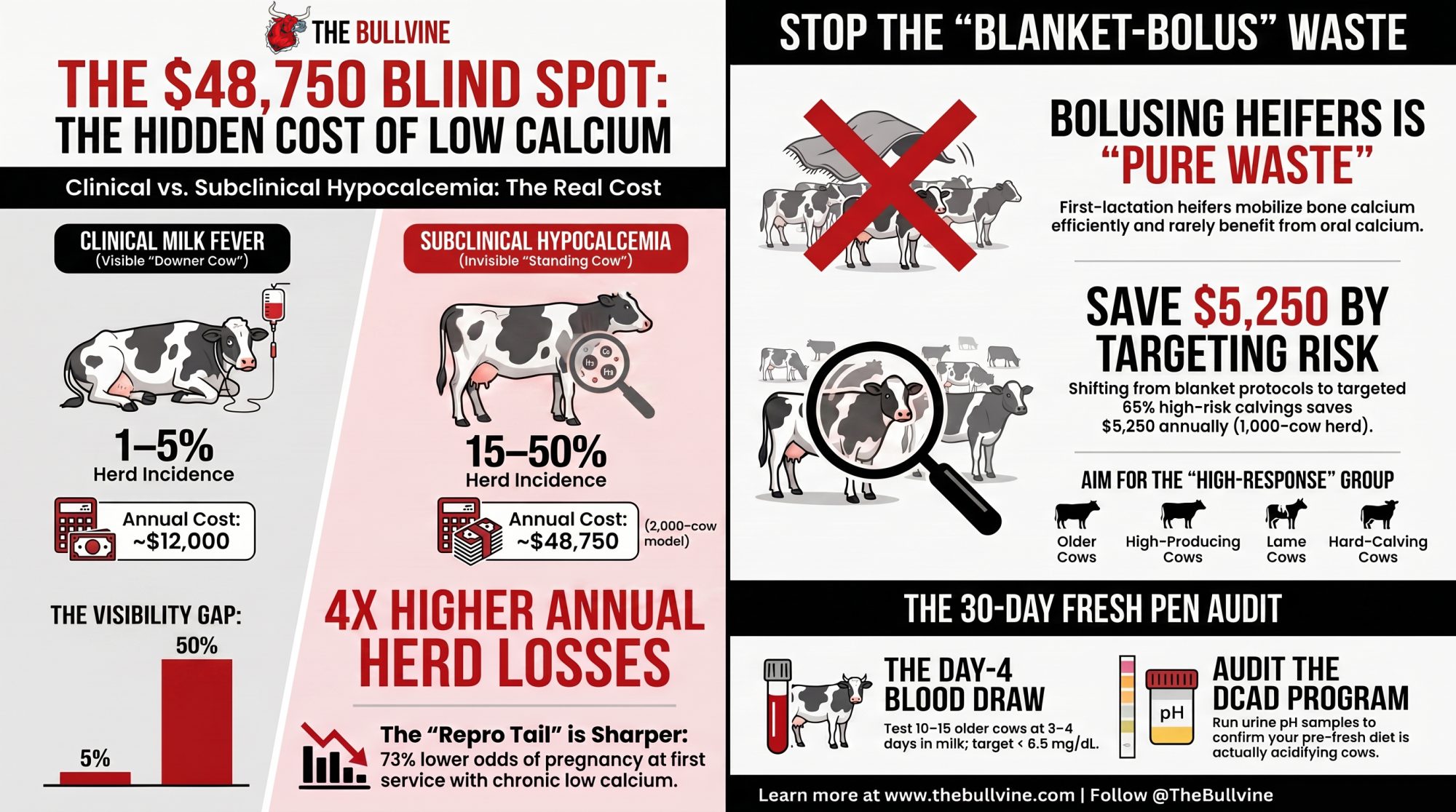
Executive Summary: About half of your mature fresh cows dip into subclinical hypocalcemia, and the modeled herd-level losses hit about four times what you’re spending on clinical milk fever. Those cows never show up on the milk-fever board, but they carry a higher risk of metritis, slower reproduction, and earlier culling — adding roughly $50 to 60 per cow in six‑month costs on top of the obvious cases. The article makes one blunt case: the number that matters isn’t your milk fever rate, it’s how many older cows are still under 8.5 mg/dL (2.12 mmol/L) on day 3–4, and whether you’re wasting bolus money on heifers that physiology says rarely need it. Using current Oetzel-style economics, blanket two‑bolus protocols in a 1,000‑cow herd can run around $15,000 a year, while targeting roughly 65% of higher‑risk calvings drops that spend to about $9,750 with better health payback. If you’re proud of a low milk fever rate but have nagging fresh‑cow disease and repro issues, this piece shows you exactly how to run a 30‑day day‑4 blood‑draw check, re‑aim calcium at high‑risk cows, and confirm whether your DCAD program is actually working.

Picture two third-lactation cows that calved overnight. Both got up fine. Both walked to the fresh pen. Neither one will ever land on your milk fever board — and one of them is quietly costing you more than the downer cow you’ve spent your whole career dreading.
That’s the uncomfortable math at the center of transition-cow management right now. The cow on the ground gets the IV bottle, the attention, and the protocol. The cow standing next to her, blood calcium sitting just under the line for three days running, gets nothing. Because nobody’s looking, and the research keeps landing in the same place: she’s the one bleeding margin out of your fresh pen — not as a scare-line, but as a number you can actively address and improve.
What’s Really at Stake
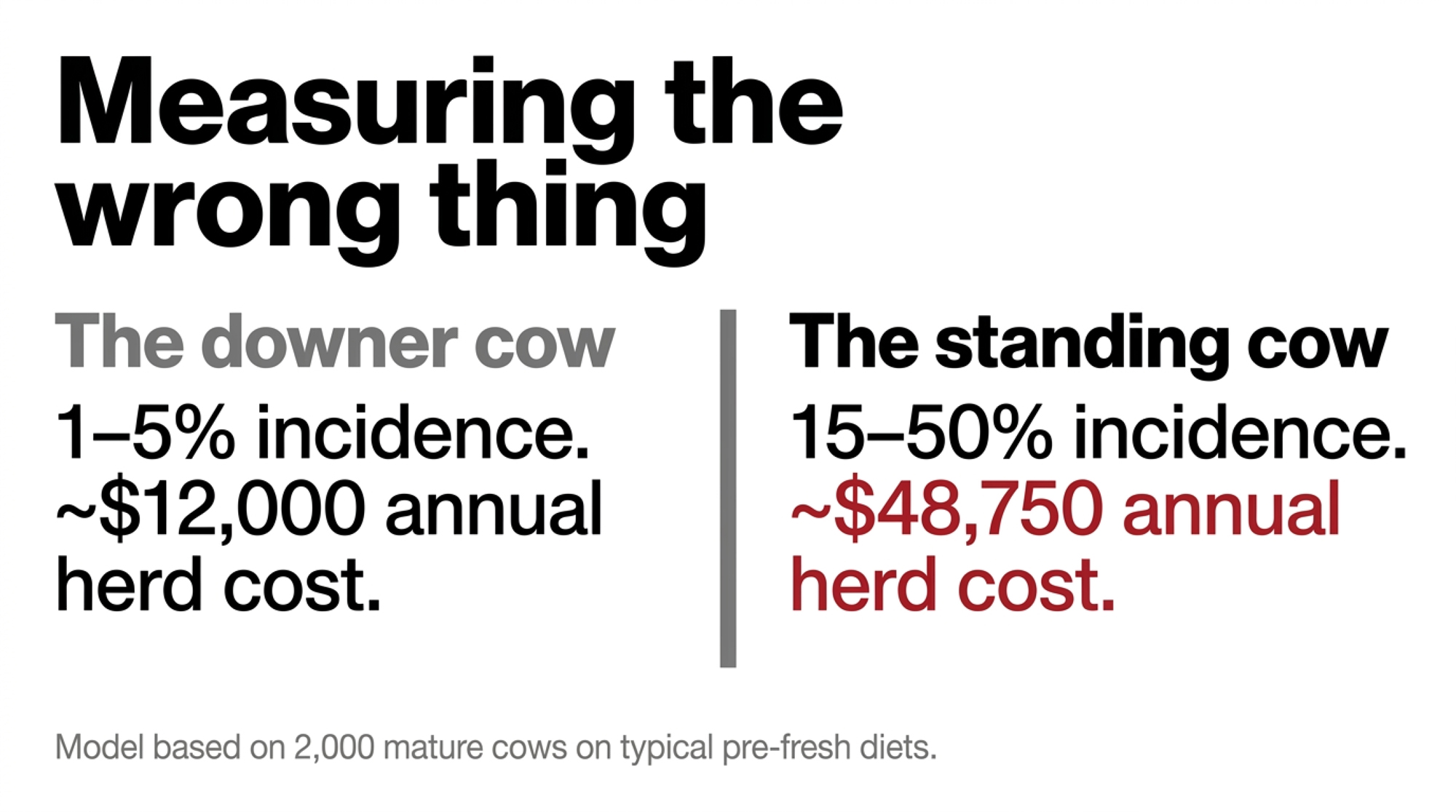
Most of us measure the wrong thing, and we were trained to do so. Clinical milk fever shows up in roughly 1–5% of cows in well-managed herds, according to the University of Wisconsin–Madison Extension and multiple veterinary summaries. It’s dramatic, it’s visible, and it’s the disaster everyone learned to fear.
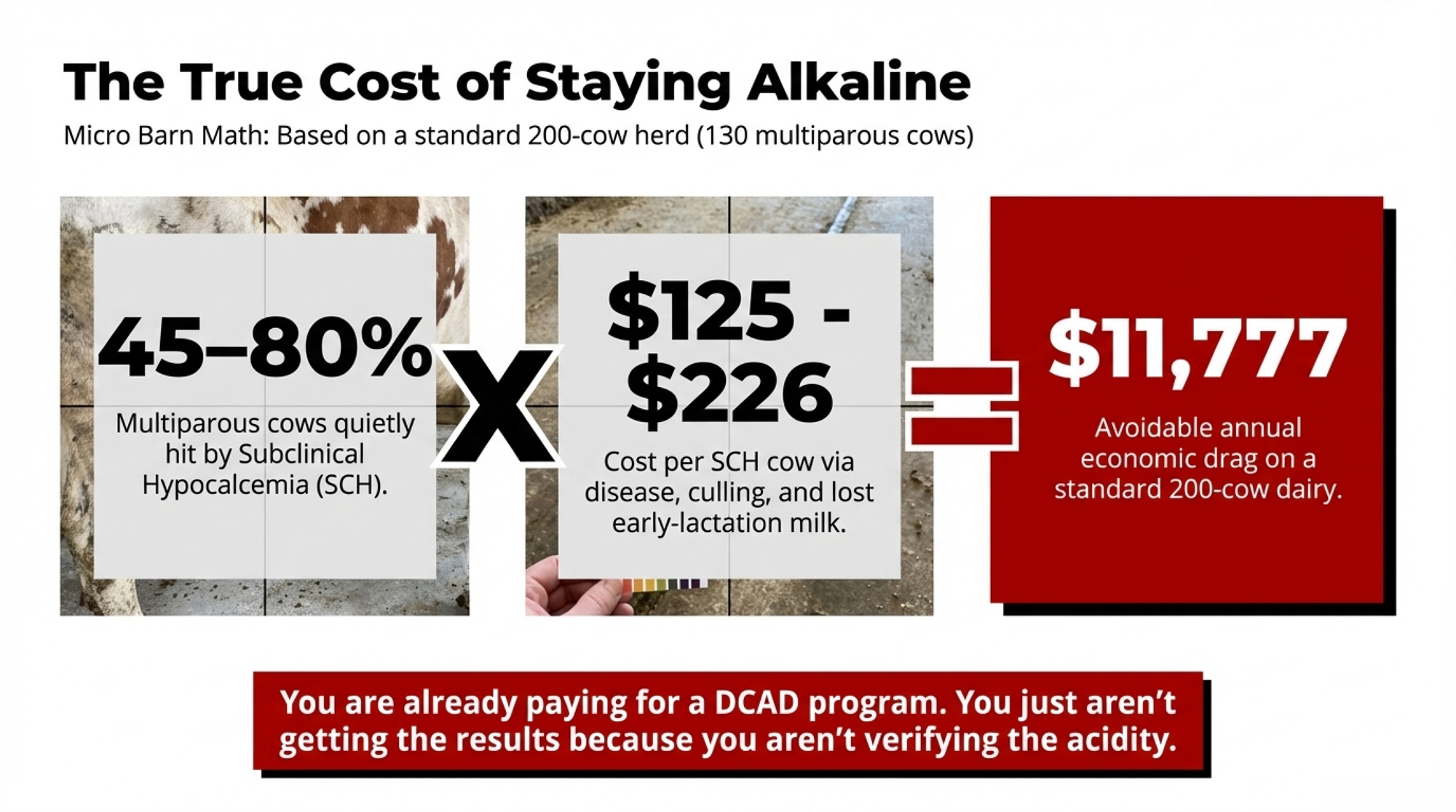
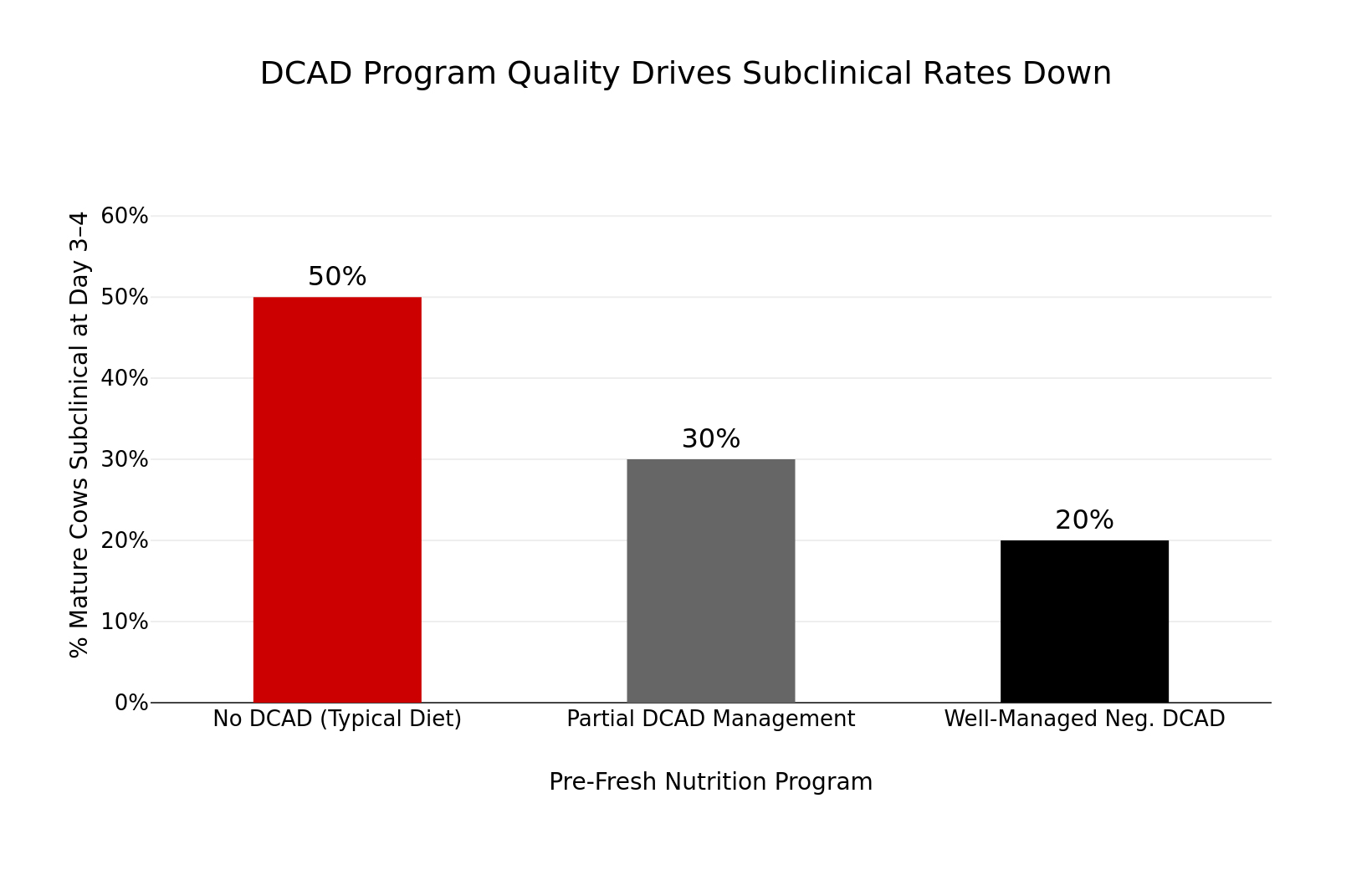
Subclinical hypocalcemia — low blood calcium with no outward signs — is a different animal. Michigan State Extension data indicate about 50% of second-lactation-and-older cows dip into it on typical pre-fresh diets, dropping to roughly 15–25% under well-managed negative DCAD programs. Here’s how the two stack up:
| Metric | Clinical Milk Fever | Subclinical Hypocalcemia |
|---|---|---|
| Incidence in mature cows | 1–5% | 15–50% |
| Visibility in fresh pen | High — cow goes down | Invisible — cow stands |
| Cost per case (USD, Oetzel modeling) | ~$300 | ~$117 |
| Est. annual cost, 2,000-cow herd | ~$12,000 | $48,750 |
| Metritis risk vs. normocalcemic | Moderate | 66–88% higher |
| First-service conception odds | Normal | OR = 0.27 (73% lower) |
| Responds to bolus protocol | Yes | High-risk cows only |
| Heifer risk level | Low-moderate | Very low — bolus wasteful |
| DCAD impact on incidence | Minimal (late-stage) | Drops to 15–25% |
*~50% on typical pre-fresh diets; 15–25% under well-managed negative DCAD. Per-case costs from Gary Oetzel’s UW–Madison modeling (2011–2013); herd-cost figures from his modeled 2,000-cow US scenario.
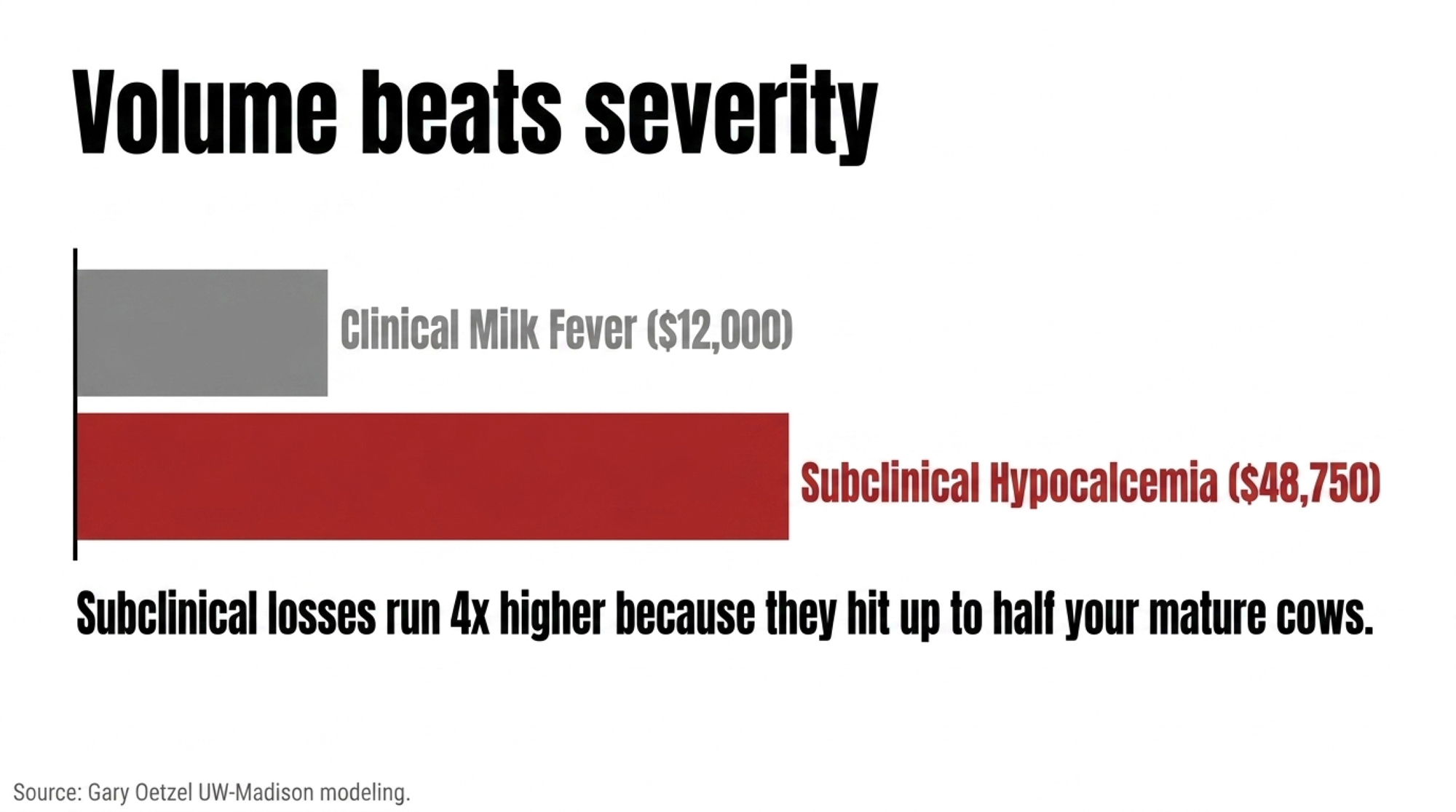
Now do the multiplication. The reason subclinical losses run roughly four times the clinical ones isn’t that each case is worse — it’s that it hits so many more cows. And remember, those per-case figures are in early-2010s US dollars; in today’s input and milk-price environment, the real gap is almost certainly wider, not narrower. European field data summarized by industry technical sources put the added cost of postpartum subclinical hypocalcemia at roughly €50–60 per cow over six months — treatment, lost milk, and reproduction — versus normocalcemic herdmates. Different currency, different continent, same direction.
If you run mostly mature cows and you’ve been quietly proud of a low milk fever rate, this is the story that should make you a little uncomfortable in a good way.
The Cow That Got Up but Never Recovered
Here’s the reframe that changes how you watch the fresh pen. The question isn’t “how many went down?” It’s “how long did calcium stay low?” Recognizing and addressing this early can make a real difference in herd outcomes and profitability.
Calcium drops around calving, bottoms out somewhere between 12 and 24 hours, and in a healthy cow starts climbing back. That recovery curve is the whole game. A Holstein cohort study, summarized by Dellait, sorted cows by the dynamics of their hypocalcemia — transient, prolonged, or delayed — and the pattern was hard to miss. Cows with only a short, transient dip adapted well and stayed relatively healthy. The cows that stayed low — prolonged or delayed — carried a higher risk of early-lactation disease, removal, and lower milk.
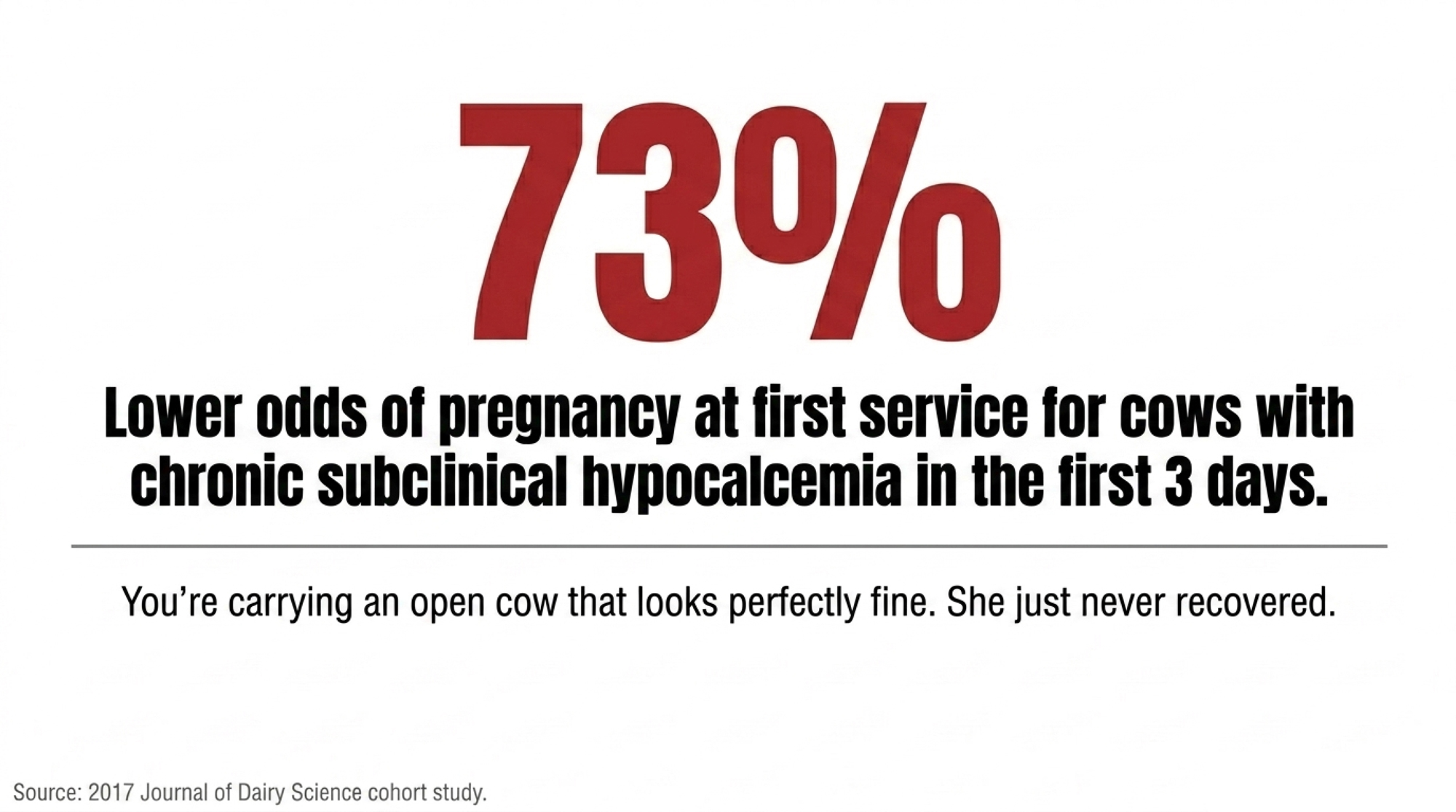
The reproductive tail is sharper still. A 2017 Journal of Dairy Science prospective cohort found cows with chronic subclinical hypocalcemia in the first three days postpartum took longer to resume ovarian activity and had about 73% lower odds of pregnancy at first service — an odds ratio of 0.27 — compared with cows that had normal calcium. That’s not a rounding error. That’s a cow you’re carrying open while she looks perfectly fine.
So you’ve got an animal that got up, walked away, and showed no signs. And she’s the slow breeder, the metritis case, the eventual cull. She just never got off the mat. You couldn’t see it because you were watching for the wrong thing.
Why Is Low Calcium Both a Cause and a Symptom?
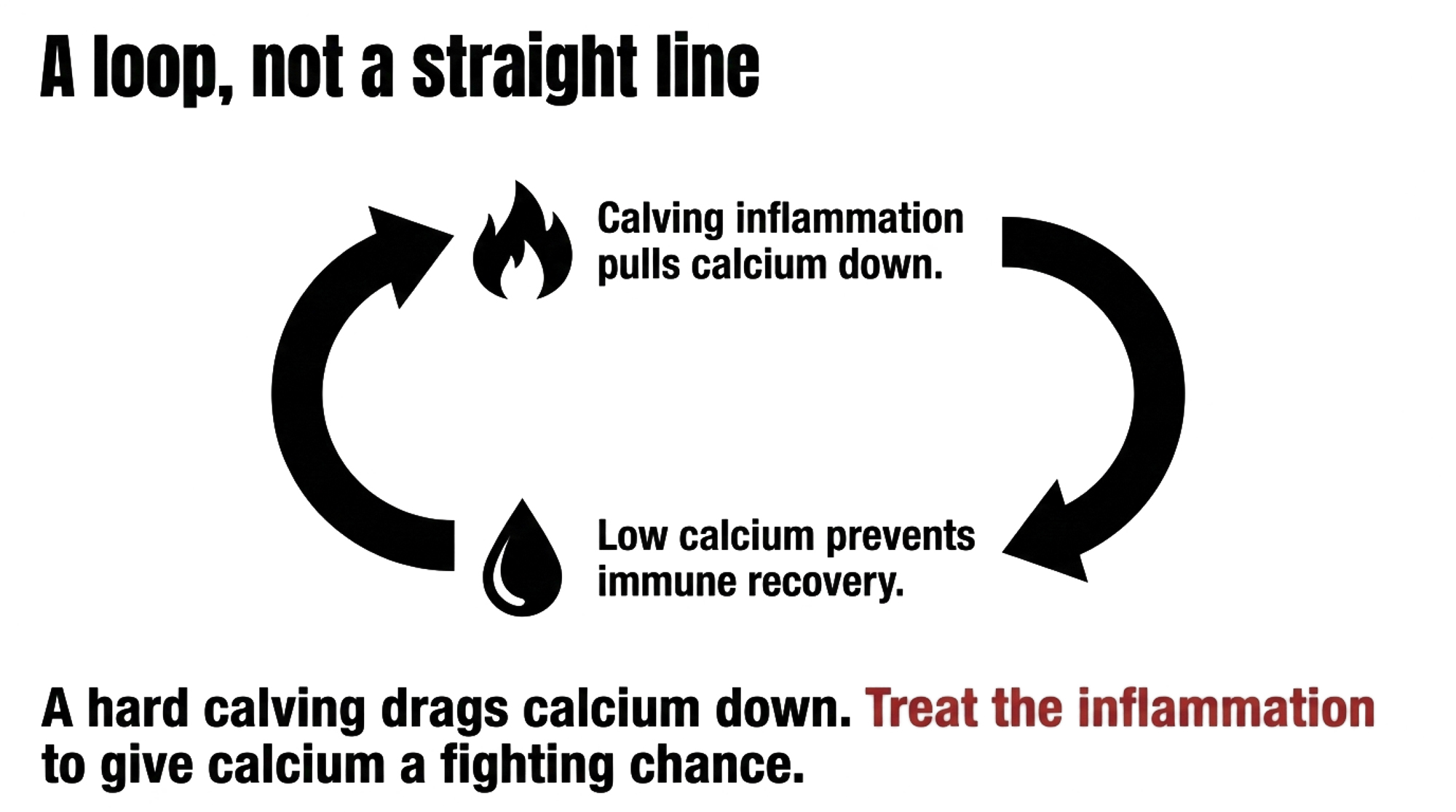
It’s tempting to read this as a straight line: low calcium causes disease. It isn’t. It’s a loop — and that two-way street is the part that often gets lost between the lab result and the fresh-pen conversation.
Think of it like a smoke alarm wired to a breaker panel. Calving lights up the immune system. That inflammatory surge pulls calcium down. And if the cow can’t reset the breaker, she stays stuck — low calcium and high inflammation feed each other. Penn State and other transition-cow researchers frame hypocalcemia and systemic inflammation as part of the cow’s normal physiology, with inflammatory markers climbing from around 14 days pre-calving, peaking at calving, then easing over the following week or two. The trouble starts when that response runs hot and long.
Recent reviews on calcium dynamics and inflammatory responses conclude that systemic inflammation is consistently associated with reduced blood calcium, and some researchers now propose immune activation itself as a root cause of subclinical hypocalcemia. A Dellait-summarized 2019 study of European commercial herds found that cows sitting at 2.5 mmol/L (about 10.0 mg/dL — the healthy end of the range) calcium on day 3 had a 66–88% lower chance of metritis than cows down at 1.5 mmol/L (about 6.0 mg/dL), depending on parity.
A hard calving, a dirty uterus, a coliform mastitis case — each one drags calcium down and makes recovery harder. That’s exactly why the fresh-cow problem list is the first place to look. Metritis cows and low-calcium cows tend to be the same cows.
The Blanket-Bolus Trap
So a producer runs a few blood draws, sees 30, 40, maybe 50% of his older cows under 8.5 mg/dL (2.12 mmol/L) — a cut-off drawn largely from Martinez’s University of Florida work, though some studies use 8.0 mg/dL (2.0 mmol/L) — and asks the obvious question: what do I do Monday? This is where a lot of farms get sold the easy answer. Bolus every cow, every calving, done.
The economics don’t back it up. A recent meta-analysis of prophylactic oral calcium found little evidence that blanket postpartum bolusing improves milk yield across the trials reviewed. A 2016 stochastic model and subsequent extension summaries showed the return lives in the high-risk cows — older, high-producing, lame — while spreading boluses across the whole herd dilutes the benefit until it disappears. A 2023 Guelph DHMCP hypocalcemia update concluded that blanket therapy isn’t beneficial, pointing instead to the cows where oral calcium earns its keep: high-producing cows, older cows, lame cows, and cows with difficult calvings.
The ROI lives in the risk profile, not in the product.
| Cow Group | Est. % of Calvings | Subclinical Risk | Bolus ROI | Annual Waste in 1,000-Cow Blanket Protocol |
|---|---|---|---|---|
| 1st-lactation heifers | ~35% | Very Low | Near Zero | ~$5,250/yr |
| 2nd-lactation cows | ~25% | Moderate | Moderate | ~$1,500/yr if well-managed |
| 3rd+ lactation cows | ~25% | High | Strong | — (keep targeting) |
| Lame cows (any parity) | ~5–10% | High | Strong | — (keep targeting) |
| Hard calvings / twins | ~5% | High | Strong | — (keep targeting) |
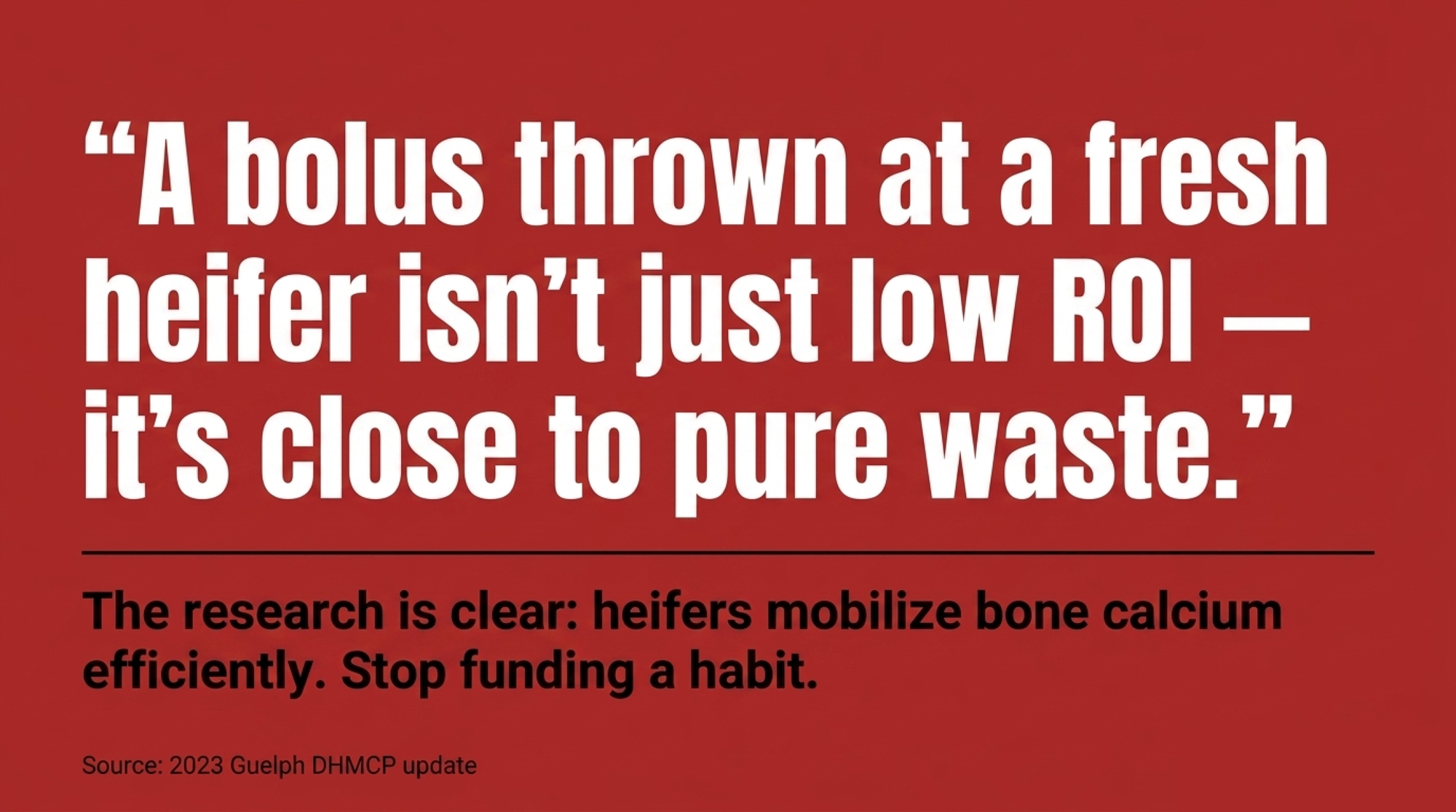
And here’s the part that should sting: first-lactation heifers are the worst possible target for a blanket protocol. They mobilize bone calcium efficiently and have a much lower risk of meaningful subclinical hypocalcemia than mature cows. So a bolus thrown at a fresh heifer isn’t just low ROI — it’s close to pure waste. You’re paying full price for a protocol most first-lactation cows never needed and won’t measurably benefit from. Multiply that by every heifer in a blanket program, and you’re funding a habit, not an outcome.
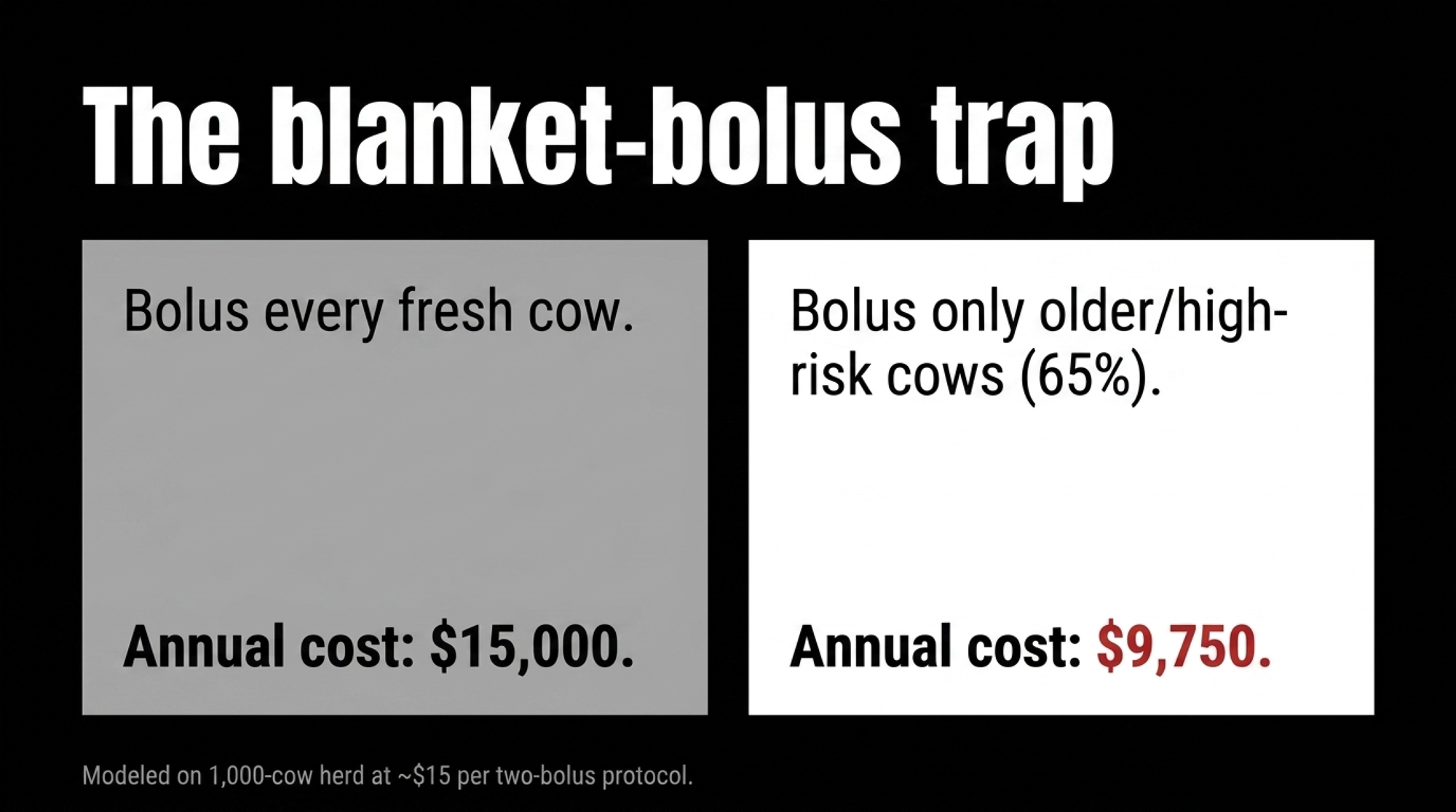
Here’s the barn math, and the point holds at whatever your boluses actually cost. Take your delivered price for a two-bolus protocol and run it two ways. Bolus every fresh cow in a 1,000-cow herd and you pay for roughly 1,000 protocols a year — a big share of them going to heifers and low-risk cows where the research shows little measurable benefit. Aim the same protocol only at your mature, higher-risk cows — say about 65% of calvings — and you’ve cut that product bill by roughly a third, with most of the remaining spend now landing where the data says it works. To put real numbers on it: at a delivered cost in the ballpark of $15 per cow for two boluses, that’s roughly $15,000 a year blanket versus around $9,750 targeted — same product, very different return, depending entirely on where you point it. Plug in your own price, and the gap moves, but the direction never does.
In lower-risk cows, the research suggests that spending buys reassurance more than results — money out the door for the feeling of having done something. Honest caveat: in herds with high subclinical rates and no DCAD program, some of Oetzel’s modeling does show blanket treatment of mature cows paying off. So the accurate line isn’t “blanket is always wrong.” It’s “blanket rarely pays in low-risk cows, or in herds already managing calcium well.”
Options and Trade-Offs for Your Operation
The story here isn’t “bolus more” or “bolus less.” It’s “measure first, then aim.” A few paths, depending on where your herd sits:
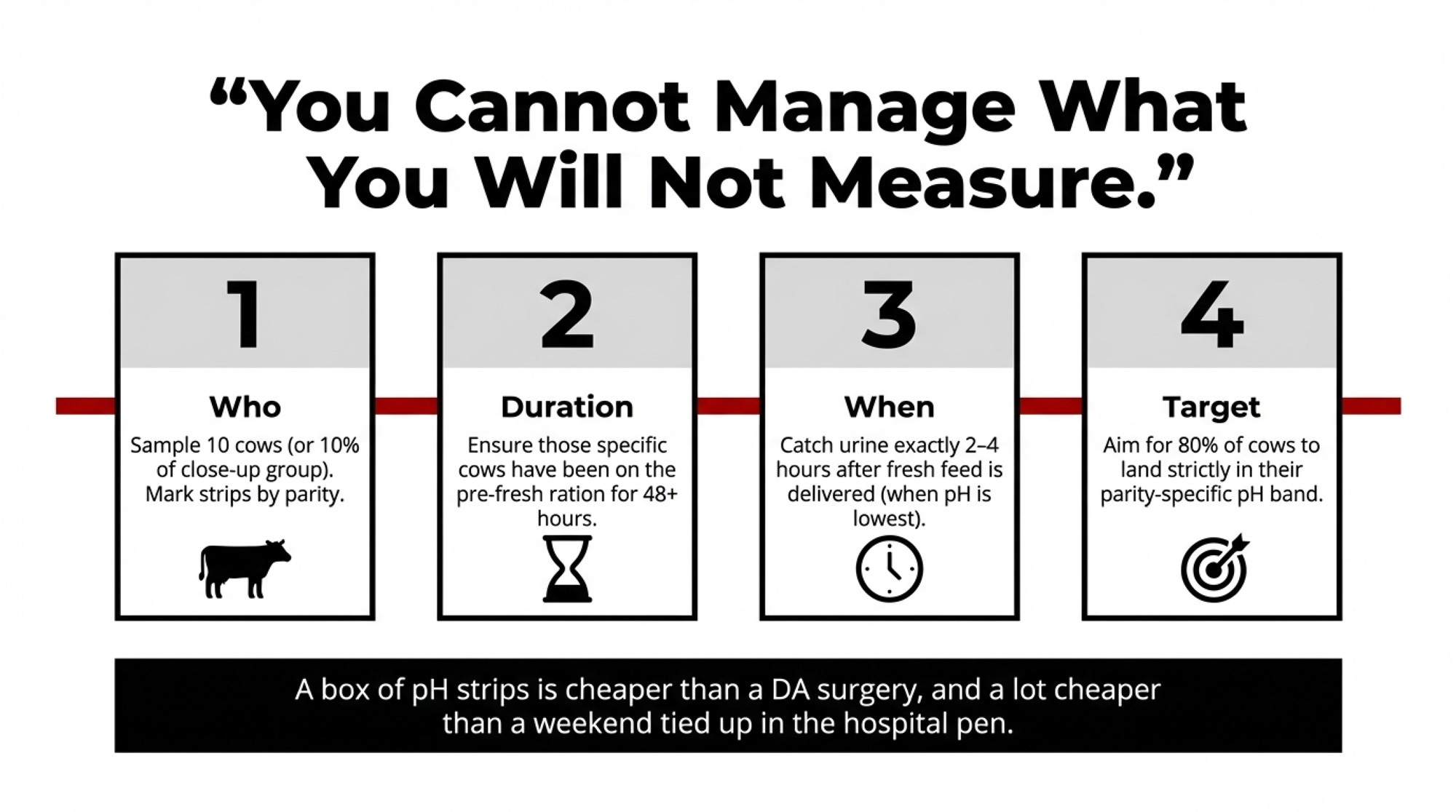
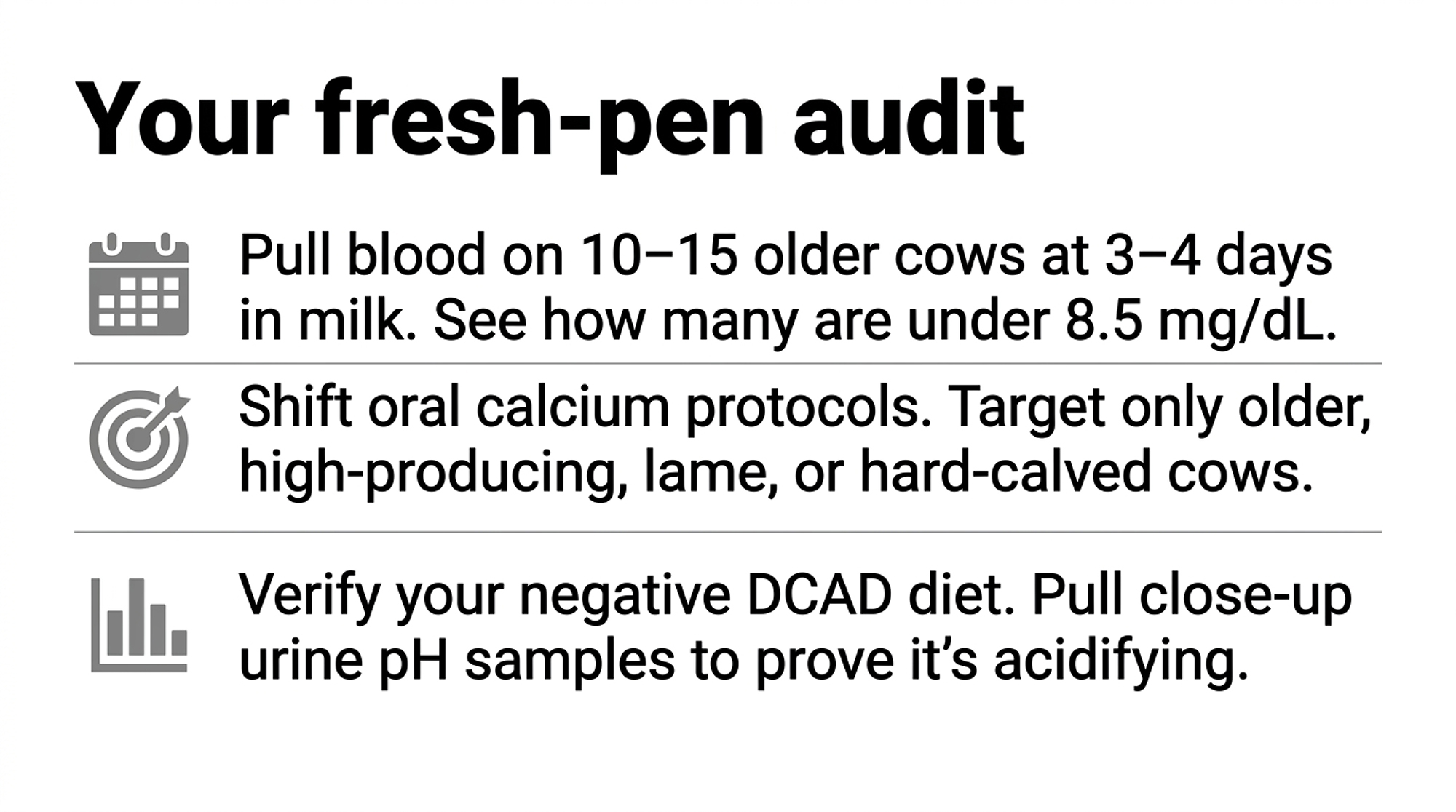
- Start with a weekly day-3-to-4 calcium check — the 30-day move. This month, work with your vet to pull blood on 10–15 second-lactation-and-older cows at 3–4 days in milk, and track the percentage still under 8.5 mg/dL (2.12 mmol/L). It’s cheap, it’s simple, and it tells you whether your current program works before you spend a dollar changing it. Where it backfires: sample sloppily or skip the repeat, and one bad week looks like a crisis.
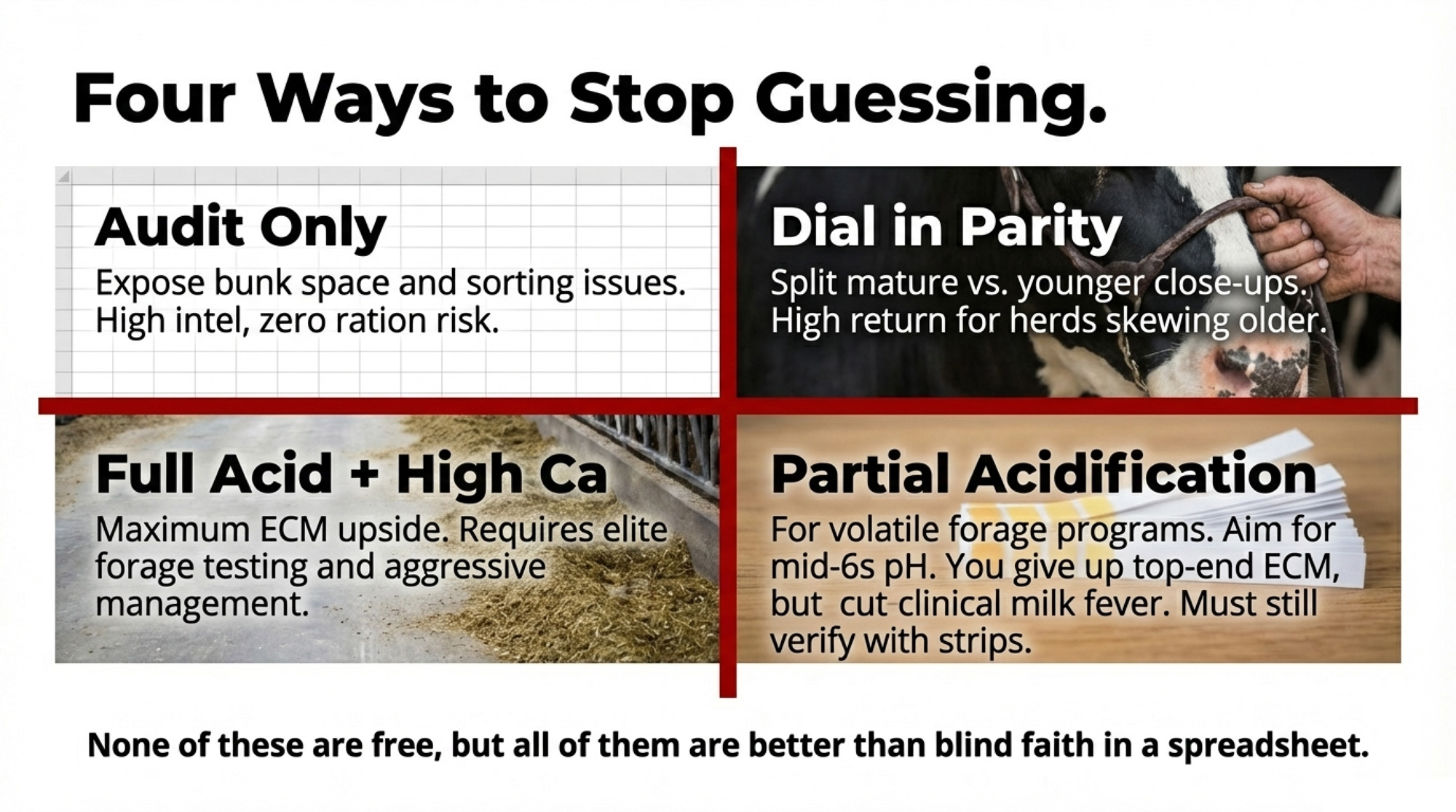
- Target oral calcium to the high-risk groups. Older cows, high producers, lame cows, hard calvings — a bolus at calving and a second 12–24 hours later. Best fit for herds with many mature cows. The risk: drifting back toward blanket habits, because targeting takes a discipline the shotgun approach doesn’t.
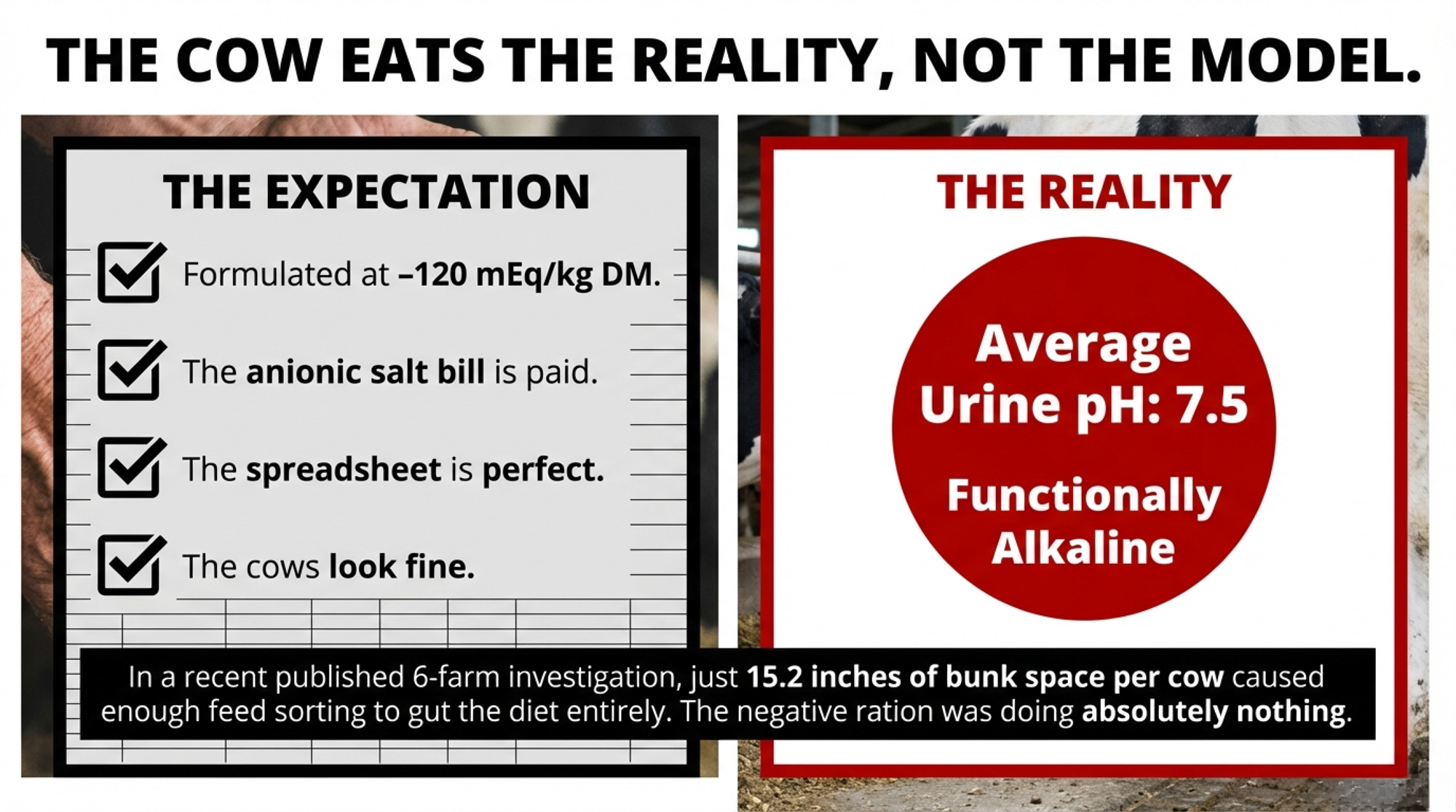
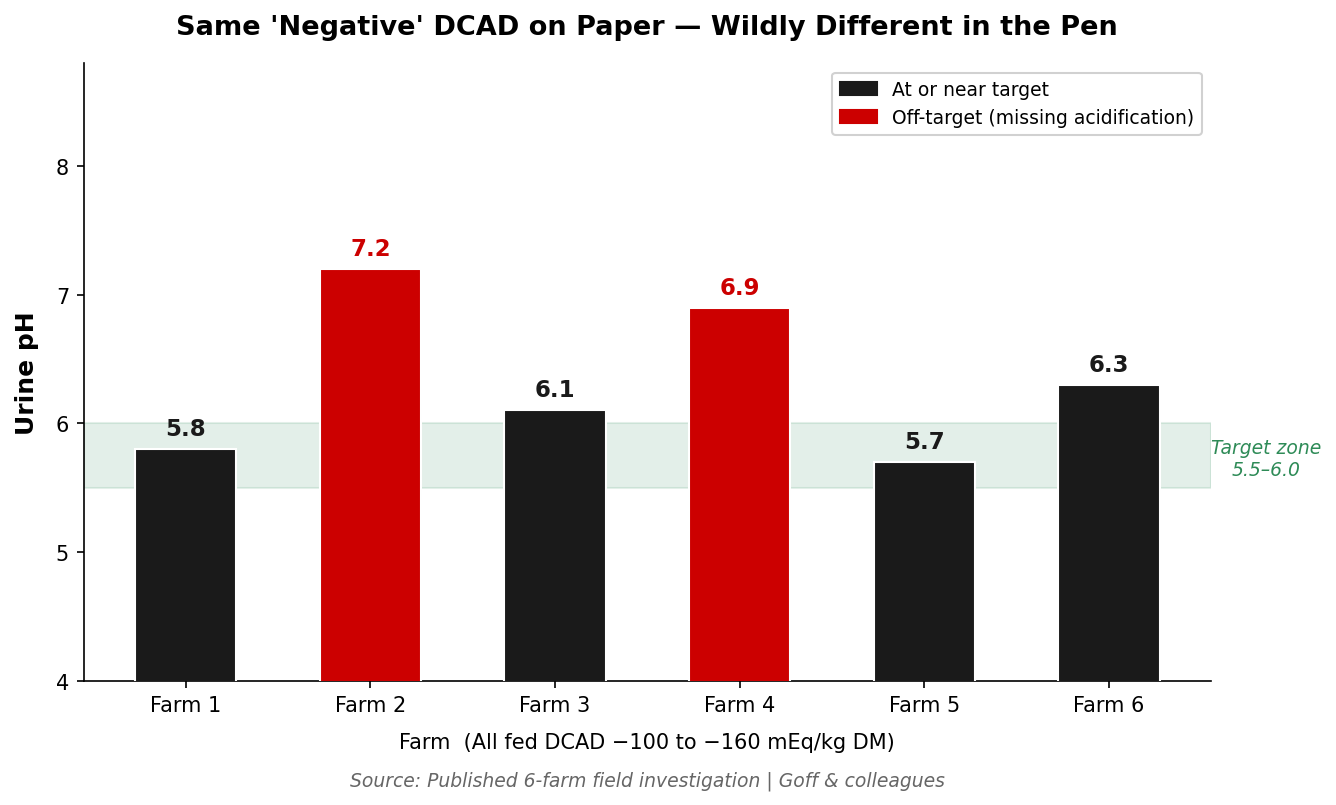
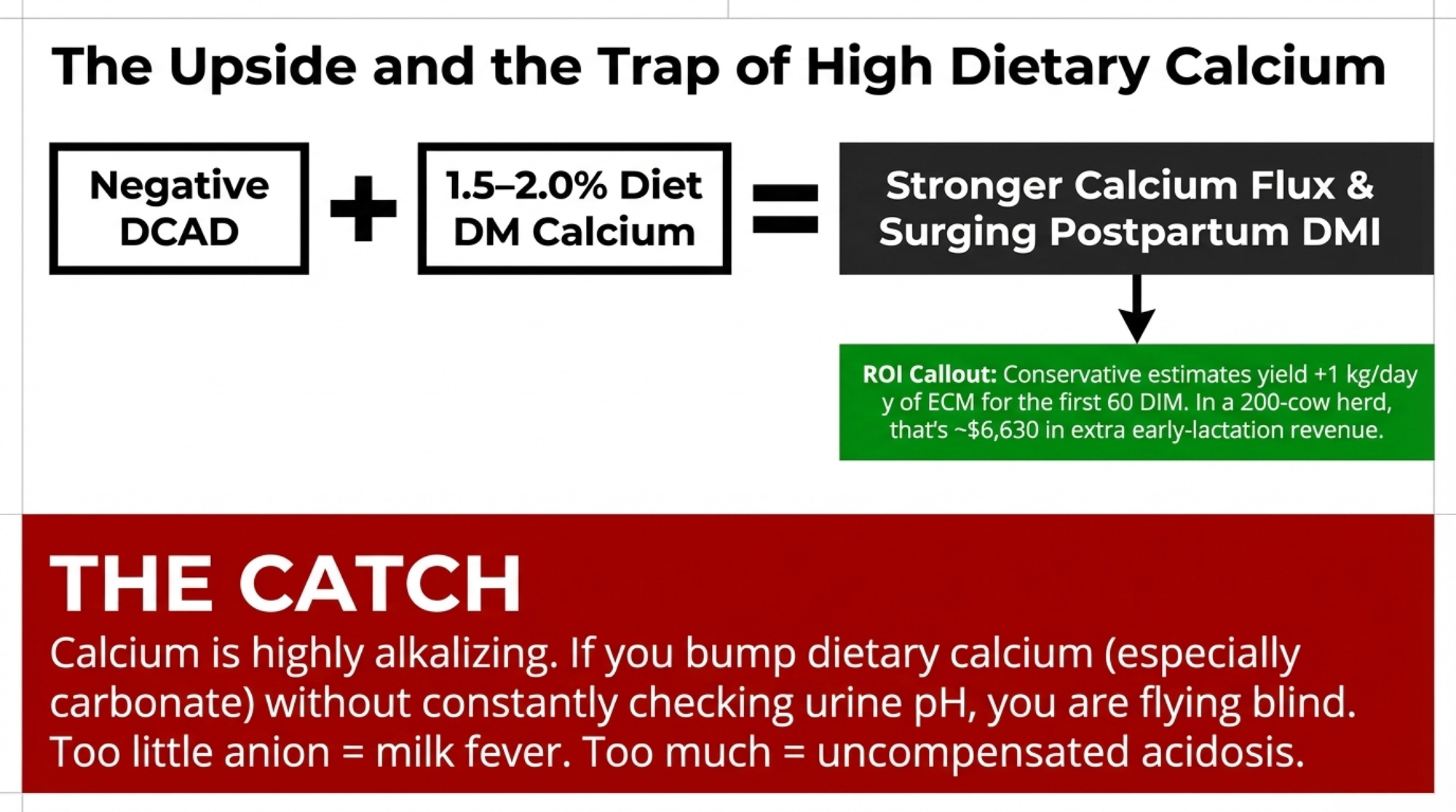
- Tighten the pre-fresh program instead of treating downstream. A well-run negative DCAD diet shrinks the low-calcium group at the source. It demands forage testing, mixing accuracy, and urine pH monitoring — a real management load. Where it backfires: a half-built DCAD program can crater intakes without ever fixing calcium.
- Manage the inflammation, not just the mineral. Cleaner calving pens, fewer hard pulls, faster response to metritis and severe mastitis. Lower the inflammatory load, and you give the cow’s own calcium recovery a fighting chance. The catch: it’s a whole-team habit change, not a line item you can buy.
Your Fresh-Pen Audit Protocol
Don’t nod along — run these checks against your own barn. Each one is a decision, not a takeaway:
- Find your real number. What percentage of your mature fresh cows are still under 8.5 mg/dL (2.12 mmol/L) at day 3–4? If the honest answer is “no idea,” that’s the gap — and the weekly blood draw on 10–15 older cows is how you close it. You’re tracking the wrong 5% until you do.
- Map your problem list to age. Pull last month’s fresh-cow cases — metritis, DAs, slow breeders. Do they cluster in your older animals? That overlap is your calcium map. And treat any hard calving, twins, or metritis case as a calcium-recovery risk, not just an infection to clear.
- Audit the spend before you buy another pail. If you’re blanket-bolusing, what’s the annual bill, and how much is landing on heifers — the one group that rarely needs it? That’s not low ROI; it’s close to pure waste.
- Confirm your DCAD actually works. If your negative DCAD program has never been urine-pH checked, you don’t yet know whether it’s acidifying cows or just looking good on the ration sheet. A handful of close-up urine pH samples settles it in a week.
- Know your high-response group. Older, high-producing, lame, hard-calved cows — are they getting targeted support today, or are they buried in a one-size-fits-all protocol?
Key Takeaways
- Subclinical hypocalcemia hits far more cows than clinical milk fever, so if you’re only watching the downers, you’re missing most of the cost.
- Day‑3/4 blood calcium on mature cows is the real fresh‑pen number; if you don’t know how many are under 8.5 mg/dL, that’s your first 30‑day job.
- Blanket bolusing burns money on heifers and low‑risk cows; aim calcium support at older, high‑producing, lame, and hard‑calved animals instead.
- A negative DCAD diet and cleaner calving management cut the low‑calcium herd at the source — but only if you’re checking urine pH to prove it’s working.

The shift here is really about a different kind of attention. For decades, the job in the fresh pen was watching for the cow that goes down. The harder, more valuable job is spotting the cow that got up and never really recovered. That’s a quieter signal, and it won’t announce itself.
So here’s the question worth carrying out to the barn Monday morning:
If you drew blood on your next fifteen older fresh cows at day four, how many do you honestly think would still be under the line — and are you ready to find out?
Run Your Numbers
Herd Health ROI Calculator — This article says undermanaged calcium quietly drives culling, metritis, and lost milk. Plug in your herd size, culling rate, and replacement cost to see what those fresh-cow losses are actually costing you—and whether tightening transition health pays before you spend another dollar on boluses.
Complete references and supporting documentation are available upon request by contacting the editorial team at editor@thebullvine.com.
Learn More
- Subclinical hypocalcemia: the day-4 fresh cow test — Harnesses rumination data as a cheap proxy to separate transient “bouncers” from persistent “flat-liners,” arming operational decision-makers with a strict protocol to stop blanket-bolusing cows that are already winning the lactation.
- The 15:1 ROI Protocol: How Anti-Inflammatory Treatment is Cutting Transition Disease in Half — Dismantles the traditional energy-balance myth by following the money on a $10 targeted anti-inflammatory strategy, positioning strategic planners to slash multi-parity fresh pen disease rates by half.
- Mastering the Transition: A Holistic Approach to Dairy Cow Health and Productivity — Delivers an unconventional, multi-pillar framework combining precision wearable sensors and staff dynamics, proving that a single extra hour of transition cow lying time dictates a 2.5% production increase.
 The Sunday Read Dairy Professionals Don’t Skip.
The Sunday Read Dairy Professionals Don’t Skip.
 The Sunday Read Dairy Professionals Don’t Skip.
The Sunday Read Dairy Professionals Don’t Skip.Every week, thousands of producers, breeders, and industry insiders open Bullvine Weekly for genetics insights, market shifts, and profit strategies they won’t find anywhere else. One email. Five minutes. Smarter decisions all week.